How to Spot Red Flags When Choosing a Clinical Fellowship Site
A setting-by-setting checklist to protect your CF from predatory SNFs, bad contracts, and inadequate supervision
By Benjamin Thompson, M.S., CCC‑SLPReviewed by SLP Editoral TeamUpdated July 18, 202625+ min read
Points of interest…
Productivity targets above 90 percent from day one signal a site that treats clinical fellows as billing units, not learners.
ASHA requires 18 hours of direct supervision across three segments, and legitimate sites exceed that minimum.
Non-compete clauses, vague termination language, and missing mentorship commitments are contract red flags worth walking away from.
If red flags surface after your CF starts, ASHA allows you to transfer sites and retain hours already completed.
A clinical fellow in San Diego recently posted to Reddit's r/slp community asking which skilled nursing facilities are predatory and which might safely support a CFY. The question came with a warning list: unrealistic productivity expectations, poor mentorship, and questionable billing practices. Within hours, the thread filled with cautionary tales from SLPs who had accepted offers too quickly, only to face lost clinical hours, ethical violations, or delayed licensure when they had to transfer sites mid-year.
The stakes are real. Accept the wrong clinical fellowship and you may find yourself working without proper supervision, pressured to document treatments you did not provide, or burning out before you earn your CCC-SLP. Many new SLPs assume red flags are obvious, but some of the most damaging issues appear only in contract fine print, billing policies, or vague promises about mentorship.
Red-flag awareness is not about fear. It is about knowing the difference between a difficult learning curve and a site that will undermine your training year.
Deal-Breaker Vs. Negotiable Red Flags: A Severity Framework
The core tension every clinical fellowship candidate faces is urgency versus safety: you want to start your CF as soon as possible, but accepting the wrong site can derail your entire path to certification. Not every red flag carries the same weight, and treating all warning signs as equal leads to either paralyzing indecision or dangerous complacency. What you need is a structured way to sort the signals so you can walk away when it matters, negotiate when there is room, and monitor when the concern is manageable.
No competitor resource systematically ranks clinical fellowship red flags by severity. The three-tier framework below is designed as a decision-making checklist you can bring to every interview, contract review, and site visit. For a broader overview of fellowship requirements, see our ASHA clinical fellowship guide.
Tier 1: Deal-Breakers (Walk Away Immediately)
These are non-negotiable. If you encounter any of the following, no salary, signing bonus, or convenient location justifies accepting the offer.
No qualified CF mentor on staff: ASHA requires your mentor to hold the Certificate of Clinical Competence in Speech-Language Pathology (CCC-SLP) for the requisite period. If the facility cannot name a mentor who meets that standard, the site cannot legally supervise your fellowship.
Pressure to bill for services not rendered: Any hint that you will be expected to document treatment minutes that did not occur, or to bill skilled therapy when maintenance-level services were provided, is an ethical and legal violation. This is not a gray area.
No plan for direct observation hours: ASHA mandates a minimum number of direct observation hours across the fellowship. If leadership seems unaware of this requirement or has no scheduling framework for observations, your hours may never be validated.
Mentor does not hold CCC-SLP for the required duration: Even if someone on staff has the CCC-SLP, confirm they have held it long enough to qualify as a mentor under current ASHA guidelines. A recently certified clinician, however talented, may not yet be eligible.
If any Tier 1 flag appears during the interview process, thank the interviewer for their time and move on.
Tier 2: Serious Concerns (Negotiate or Get Written Assurances)
These issues are significant but potentially resolvable if the employer is willing to put commitments in writing before you sign.
Productivity expectations above 85 percent: Productivity targets in the mid-to-high 80s are common in skilled nursing facilities, but expectations that push toward 90 percent or higher from the start of your fellowship leave almost no time for documentation, mentorship, or learning. If the site quotes a number above 85 percent, ask whether a ramp-up period is built in and get the answer in your contract.
Sole-SLP staffing with no backup: Being the only speech-language pathologist at a facility is challenging under any circumstances, but it becomes precarious during a CF. If you are sick, overwhelmed, or facing a clinical situation beyond your training, there should be a concrete plan for coverage and consultation.
Non-compete clauses with a broad geographic radius: Some contracts include non-compete language that could prevent you from working within a wide area for a year or more after leaving. Before signing, ask for specifics on the radius, duration, and enforceability in your state.
Vague contract language on supervision: Your contract should spell out the frequency, format, and duration of supervision sessions. Phrases like "mentorship will be provided as needed" offer no guarantee. Push for explicit terms: weekly meetings, monthly direct observations, and a named mentor.
Any Tier 2 concern that the employer refuses to address in writing should be treated as a Tier 1 deal-breaker.
Tier 3: Yellow Flags (Monitor but Not Disqualifying)
Yellow flags are worth noting and watching, but on their own they do not justify turning down an otherwise strong offer.
High caseload within industry norms: A caseload at the upper end of what is typical for the setting is not ideal, but it is common. Track your workload from the first week and raise concerns early if it climbs beyond sustainable levels.
Limited CEU support: Some employers offer generous continuing education budgets; others do not. Limited CEU funding is inconvenient, not dangerous, and many affordable or free options exist.
Informal but present mentorship structure: A mentor who keeps an open-door policy rather than scheduling rigid check-ins can still provide excellent guidance. The key question is whether mentorship actually happens, not whether it follows a formal template.
Using the Framework
Print or save this three-tier checklist before you begin interviewing. Prepare targeted questions for each tier using our SLP job interview questions resource. During each site visit, mentally (or literally) check items against the tiers. If a Tier 1 flag appears, stop evaluating and decline. If Tier 2 concerns arise, draft specific questions and follow up in writing. If only Tier 3 flags surface, weigh them against the site's strengths and make a confident decision. This framework puts you in control of a process that too often feels like it is happening to you rather than for you.
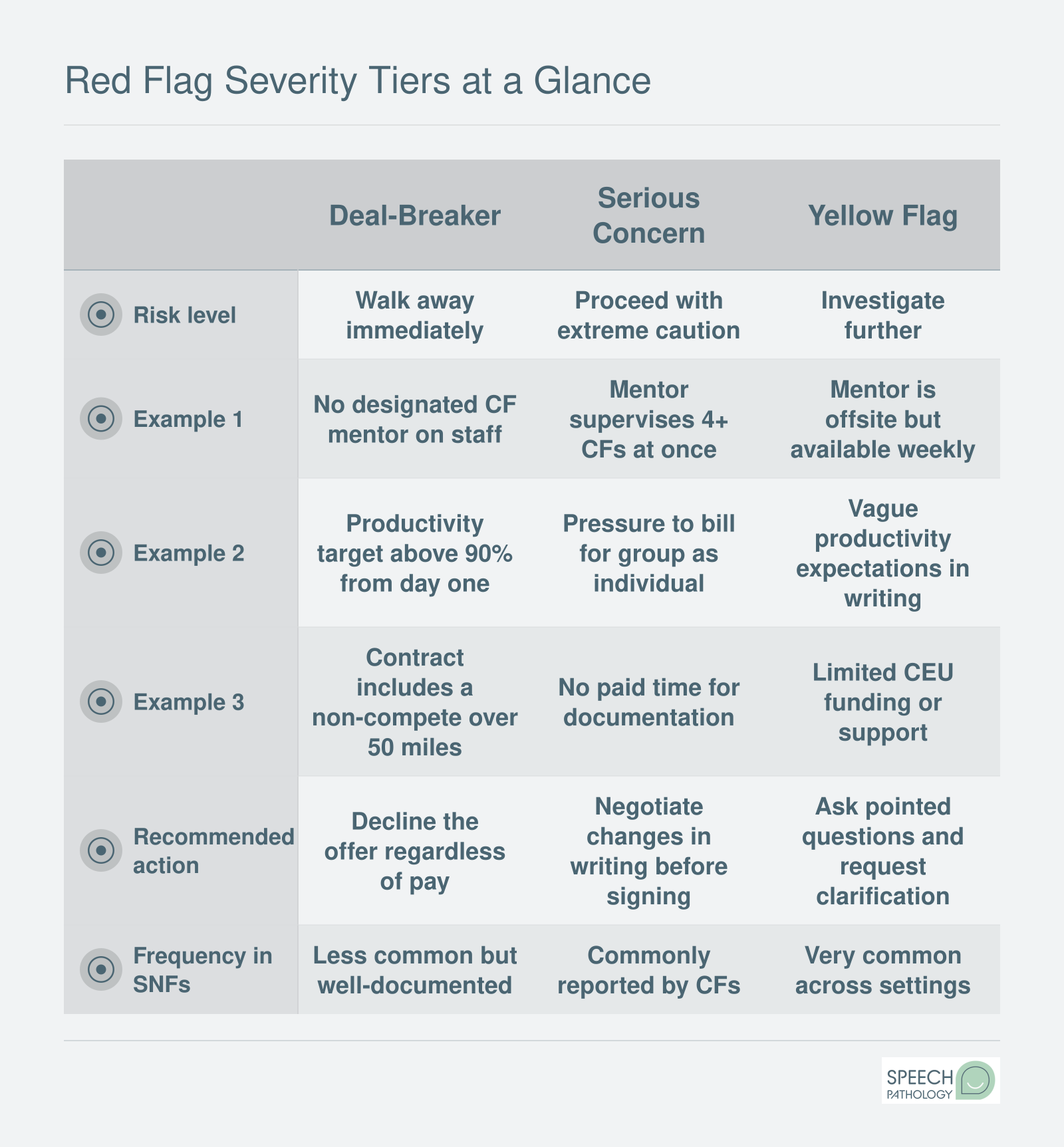
Red Flag Severity Tiers at a Glance
Not every red flag carries the same weight. Use this framework to quickly classify concerns you encounter during your clinical fellowship search. Screenshot it, save it, and reference it when evaluating offers.
Snf-Specific Red Flags: Productivity Benchmarks, Billing Pressure, and Staffing
Skilled nursing facilities can offer clinical fellows genuine clinical variety, a fast caseload, and strong mentorship. They can also be environments where new SLPs are handed unrealistic expectations before they have finished orienting. Knowing the difference starts with understanding what reasonable productivity actually looks like in this setting.
What Productivity Numbers Actually Mean
In an SNF, productivity refers to the percentage of your paid workday spent in billable direct patient care.1 Experienced SLPs in skilled nursing typically work in the 75 to 80 percent range, with some high-performing clinicians reaching 80 to 85 percent. Anything above 85 percent for an experienced clinician consistently raises concerns in the field.1
For a clinical fellow, those numbers should be lower, not higher. A reasonable starting point is somewhere in the 60 to 70 percent range, with gradual growth toward 60 to 75 percent as you build efficiency and caseload familiarity. Reaching 75 to 80 percent by the later months of your fellowship is considered high but achievable.1 If a facility expects you to hit 80 percent or more from your very first week, that expectation does not reflect the learning curve of a CF. It reflects a staffing model that treats you as a full-time revenue source the moment you walk through the door.
This concern shows up repeatedly in professional communities. A post on the r/slp subreddit from a clinical fellow seeking placement in San Diego put it plainly: unrealistic productivity demands and questionable ethics were the primary worries about SNF placements. That post resonated with many respondents, and for good reason. These are not isolated complaints.
The Sole-SLP Problem
One of the clearest structural red flags in any SNF is being the only SLP in the building. When you are the sole speech-language pathologist on site, there is no peer to consult when a patient presents an unfamiliar swallowing pattern. There is no coverage when you are sick, which creates informal pressure to come in anyway. Most critically, there is often no qualified mentor nearby, which can compromise the supervision structure your CF requires.
Ask directly during the interview: how many SLPs are on staff, and who will be your primary supervisor? If the answer suggests you will be largely on your own, factor that into your decision carefully. Preparing strong questions ahead of time, like those in our guide to SLP interview questions and answers, can help you uncover staffing realities before accepting an offer.
Billing Pressure and Ethical Warning Signs
Productivity pressure is not always explicit. Sometimes it shows up in subtler forms that carry serious ethical weight:
Caseload inflation: Being encouraged to keep patients on your caseload beyond what their clinical progress supports, so that billable units remain high.
Group billed as individual: Providing group therapy sessions while documenting them as individual treatment, which constitutes fraudulent billing.
RUG-level pressure: Being nudged to document in ways that push patients into higher reimbursement categories regardless of clinical need.
None of these practices are ambiguous. They expose you to professional and legal liability at a stage in your career when your license is brand new and your ability to push back is limited. If a supervisor or rehab director makes any of these expectations feel routine during the interview, treat it as a signal about the facility's broader culture.
Contracted Rehab Companies vs. Facility-Employed SLPs
Many SNFs do not employ their therapy staff directly. Instead, they contract with a rehab company, which then places SLPs and other therapists in the building. This model is not automatically problematic, but it adds a layer of accountability that can complicate your CF experience.
When you work under a contracted rehab company, your productivity targets, documentation requirements, and scheduling expectations may come from the company rather than the facility. Your supervisor may split time across multiple buildings, limiting the hands-on mentorship time your fellowship requires. In a facility-employed model, the SLP is more directly tied to the facility's patient outcomes, which can align incentives more naturally with good clinical care. Understanding how different SLP career settings shape day-to-day expectations will help you evaluate these trade-offs more clearly.
During your site evaluation, ask who sets the productivity expectations, who your supervisor's employer is, and how many sites that supervisor covers. The answers will tell you a great deal about how much support you can realistically expect.
Questions to Ask Yourself
Will I be the only SLP in the building, and if so, who covers my caseload when I'm out?
Solo coverage means no peer to consult on a tricky dysphagia eval and no backup when you're sick. ASHA requires real-time mentor access during your fellowship, so a lone-SLP site needs a clear plan for both.
Has the recruiter put a specific productivity target in writing?
Vague answers like "it depends on census" often signal expectations above 90% once you start. Get the number in your offer letter so you can compare it against realistic benchmarks before you sign.
Can I speak with a current or former fellow at this facility first?
If the company won't connect you with someone who has completed a fellowship there, treat that as data. Past fellows can tell you whether mentorship, billing pressure, and ethics matched what the recruiter promised.
Red Flags in Schools, Hospitals, and Outpatient Settings
Every clinical fellowship setting carries its own version of warning signs. While SNFs often dominate red flag discussions, schools, hospitals, and outpatient clinics each present distinct challenges that can undermine your professional development. Before accepting any CF offer, compare these setting-specific concerns so you know exactly what to watch for.
Setting
Caseload Red Flag
Supervision Concern
Contract Pitfall
Common Ethical Issue
SNF (Skilled Nursing Facility)
Productivity targets above 85 to 90 percent from the start, with little ramp-up time for new CFs
Supervisor may oversee multiple buildings, limiting direct observation and feedback
Non-compete clauses that restrict future employment in a wide geographic area
Pressure to bill for services that may not be medically necessary or to upcode treatment minutes
School
Caseloads exceeding 75 or more students, leaving minimal time for individualized therapy or documentation
Supervisor may be a special education administrator rather than a licensed SLP, reducing clinical mentorship quality
Contracts that require summer work without additional compensation, or that lock you into multi-year commitments
Being asked to reduce or deny services outlined in a student's IEP due to staffing or budget constraints
Hospital (Acute or Rehab)
Rapid patient turnover with little time allotted for thorough evaluations, especially for complex cases like dysphagia
Limited SLP-specific mentorship if the rehab department is small or if your supervisor primarily oversees other disciplines
Short-term contracts with minimal benefits, or per diem arrangements that offer no guaranteed hours
Pressure to discharge patients before they have met functional goals, driven by insurance or length-of-stay policies
Outpatient Clinic
High daily patient volume with back-to-back sessions and no built-in time for documentation or preparation
Supervision sessions that are frequently canceled or shortened due to the clinic's scheduling demands
Unpaid productivity time, where documentation, treatment planning, and report writing fall outside compensated hours
Marketing-driven treatment plans that prioritize session volume over evidence-based clinical outcomes
Contract and Legal Red Flags Every CF Should Know
Your clinical fellowship contract is a legally binding document, and the language buried in its pages can affect your career mobility, your finances, and your ability to seek recourse if things go wrong. Before you sign anything, understand these common contract provisions and why some of them should give you serious pause.
Non-Compete Clauses
Non-compete agreements restrict where you can work after leaving an employer. In the healthcare sector, these clauses typically define a geographic radius of 25 to 50 miles and a duration of one to two years. As of 2022, roughly 11.4 percent of U.S. adult workers were bound by a non-compete2, and the prevalence runs even higher among healthcare professionals such as physicians (estimated at 37 to 45 percent).1 While clinical fellows may encounter non-competes less often than physicians do, they do appear in SLP contracts, sometimes introduced right at the start of the fellowship.3
Enforceability varies dramatically by state, and SLP state licensing overview pages can help you understand your jurisdiction's regulatory landscape. Some states have moved to ban or severely limit non-compete agreements outright.3 At the federal level, the FTC approved a rule in April 2024 that would have broadly restricted non-competes, but a court injunction in July 2024 paused implementation.1 The legal landscape remains unsettled heading into 2026, so you should never assume a non-compete is unenforceable simply because you have heard they are "going away." ASHA has encouraged audiologists and speech-language pathologists to review non-compete provisions carefully.3 If your contract contains one, consult an employment attorney who practices in your state.
Sign-On Bonus and Repayment Clawbacks
Sign-on bonuses for CFs commonly range from $3,000 to more than $10,000, but the repayment terms deserve close scrutiny. Many contracts require full repayment if you leave before a specified date, sometimes within 18 to 24 months. That means if the site turns out to be a poor fit at month six, you could owe the entire amount back.
Negotiate a pro-rated repayment schedule before you sign. Under a pro-rated structure, the amount you owe decreases each month you stay, so leaving at month 12 of an 18-month commitment might require you to repay only one-third of the bonus. Employers who refuse any pro-rating may be counting on the clawback as a retention tool rather than offering a genuine incentive.
PRN Arrangements Disguised as Fellowship Positions
Some employers offer per-diem or PRN positions and market them as clinical fellowship opportunities. This is a significant red flag. PRN schedules fluctuate week to week, making it difficult to accumulate the minimum hours ASHA requires for fellowship completion within a reasonable timeframe. Beyond the hours problem, PRN positions rarely include health insurance, paid time off, or other benefits. If an offer does not guarantee a consistent, full-time schedule in writing, ask the employer exactly how your fellowship hours will be met and what happens if patient census drops.
Mandatory Arbitration Clauses
A mandatory arbitration clause requires you to resolve disputes through private arbitration rather than the court system. These provisions can limit your ability to pursue legal remedies, restrict the damages you can recover, and prevent you from joining collective actions with other employees. Arbitration is not inherently harmful, but you should understand what rights you are waiving. If you see this clause, ask whether it covers all disputes or only certain categories, and find out who selects and pays for the arbitrator.
Get a Professional Review Before You Sign
A contract that looks routine may contain language with lasting consequences. At a minimum, have an experienced mentor, ideally one who has navigated the CF process, read through every provision. For contracts that include restrictive covenants, repayment clauses, or arbitration language, an employment attorney is worth the investment. Many offer flat-fee contract reviews that cost far less than the financial exposure you accept by signing blind. Understanding how CCC-SLP certification fits into your longer-term career plan can also help you evaluate whether a restrictive contract is worth the trade-off.
Resources from ASHA on non-compete considerations for SLPs and audiologists, along with general guidance on early warning signs in new SLP positions, can help you build a checklist of what to look for. The goal is not to approach every offer with suspicion but to enter your fellowship with your eyes open and your interests protected.
How to Evaluate Supervision and Mentorship Quality
Eighteen hours of direct supervisory activities across three segments represent ASHA's minimum threshold for clinical fellowship supervision, and that baseline may not be enough to build confident, independent practice.1 ASHA requires at least six hours of direct observation per segment, totaling 18 hours across the 36-week fellowship, alongside 18 hours of indirect activities such as case discussion and chart review. Your mentor must hold the CCC-SLP for at least nine months before supervising you, complete two continuing-education hours in supervision, and submit a mentoring plan at the outset.2 These structural minimums, however, say nothing about the quality of feedback, the mentor's availability, or whether you will actually gain the skills you need to thrive after SLP certification.
What Quality Mentorship Looks Like Beyond the Minimums
A strong CF mentor schedules weekly one-on-one meetings, not sporadic check-ins squeezed between patients, and provides structured feedback on clinical reasoning, documentation, family counseling, and treatment planning. Look for mentors willing to co-treat during your first few weeks, gradually stepping back as your confidence grows. Progressive independence is the hallmark of good supervision: you should feel challenged but supported, not thrown into complex cases without scaffolding or micromanaged through tasks you have already mastered. Ask whether the mentor has supervised previous clinical fellows and what their completion rate is. If a facility cannot or will not share that data, consider it a yellow flag.
State-Level Variations in Supervision Requirements
ASHA sets the floor, but some states layer additional requirements on top. Illinois, for example, requires both ASHA CCC-SLP and an active Illinois SLP license, along with the same nine-month holding period and two supervision continuing-education hours.1 Certain states mandate on-site supervision for the majority of direct observation hours, while others permit telepractice supervision under specific conditions. Before accepting an offer, verify your SLP license requirements by state; what is acceptable in California may not satisfy Texas or New York requirements. State boards often publish CF supervisor eligibility criteria on their websites, and many offer email or phone support for clarifying gray areas.
Verification Steps and Contingency Planning
Check your prospective mentor's CCC-SLP status on ASHA ProFind before signing any contract. The database shows certification status and issue date, helping you confirm they meet the nine-month minimum.2 Ask the facility directly for its CF completion rate over the past three years and whether any clinical fellows have transferred or extended their fellowships. If your mentor leaves mid-fellowship due to resignation, medical leave, or termination, ASHA allows a new mentor to step in, but the facility must submit an updated mentoring plan and the new supervisor must also meet all qualifications. Clarify the facility's contingency protocol in writing during contract negotiations, including whether you would be granted additional unpaid time to complete supervision hours or whether a backup mentor is already identified. A facility that responds defensively to these questions may not prioritize your professional development.
ASHA CF Supervision Requirements at a Glance
ASHA sets specific supervision minimums to protect clinical fellows and ensure quality mentorship throughout the fellowship experience. Knowing these numbers before you sign a contract helps you spot sites that may fall short of compliance.
Questions to Ask Before Accepting a CF Offer
Arriving at an interview without a prepared list of questions is one of the most common ways new SLPs end up in a CF site that does not serve them. Treat this section as a printable checklist: bring it to every interview, whether in person or virtual, and use the acceptable-answer ranges to gauge what you are hearing in real time. For broader preparation advice, see our SLP internship and externship guide.
Supervision Structure
The mentoring arrangement is the core of your fellowship experience, so probe it directly.
Who will be my primary supervisor? Acceptable: a CCC-SLP who holds or is actively pursuing CF mentor credentials and has a defined availability schedule. Red flag: a vague answer like "whoever is available that day."
What happens if my mentor leaves mid-fellowship? Acceptable: a written contingency plan naming a backup supervisor. Red flag: "We'll figure it out."
Can I review the mentoring plan before I sign? Acceptable: yes, with a plan already drafted. Red flag: hesitation, delay, or a claim that the plan is created after you start.
How many CFs have completed the full fellowship here in the last three years? Acceptable: a specific number with context. Red flag: an inability or unwillingness to answer.
Productivity and Caseload
Productivity pressure is the top complaint among SNF clinical fellows, so get specifics on paper.
What is your productivity expectation during the first three months? Acceptable: 70 to 80 percent, ramping toward 85 percent as you learn the workflow. Red flag: 90 percent or higher from week one.
What does the caseload typically look like for a new CF? Acceptable: a realistic patient volume with detail on complexity. Red flag: a number that would challenge an experienced SLP.
Is productivity tied to pay, bonuses, or continued employment? Acceptable: transparent explanation of any incentive structure. Red flag: productivity minimums framed as a condition for keeping the position.
Contract and Ethical Culture
Paper and culture questions reveal how a site treats its staff when no one is watching. Understanding ASHA CF requirements ahead of time will help you spot contract language that contradicts fellowship standards.
Can I speak with a current or former CF before I accept? Acceptable: yes, with contact information offered willingly. Refusal to connect you with anyone is a red flag on its own.
Are there non-compete or repayment clauses in the contract? Acceptable: full disclosure with time to review with an attorney. Red flag: pressure to sign quickly or minimizing the significance of repayment terms.
How does the team handle situations where a patient's documented need conflicts with what a payer will cover? Acceptable: a clear, ethics-grounded answer. Red flag: an evasive response or one that signals documentation practices are driven by billing rather than patient welfare.
Print this list, circle the answers that fall in the red-flag range, and count how many you circle before you accept any offer. One or two negotiable concerns may be manageable; several deal-breakers in the same interview is a clear signal to keep looking.
Did You Know?
Clinical fellows are still in a training year, building diagnostic reasoning, treatment planning, and documentation fluency. A site that sets productivity at 90 percent or higher from day one views you as a billing unit, not a developing clinician. Legitimate employers ramp expectations gradually, honoring the fellowship as a bridge between student and independent practice.
What to Do if You Discover Red Flags After Starting Your CF
A Clinical Fellowship transfer is the process of leaving one CF site and continuing your remaining hours at a new employer, with ASHA recognizing the work you already completed. Many CFs feel trapped once they start, believing they must endure a problematic placement to finish their hours. This fear is understandable but misguided. Staying at a site with serious red flags, such as inadequate supervision or pressure to engage in questionable billing practices, can result in something far worse than the inconvenience of transferring: invalidated hours that force you to start over entirely.
Your Completed Hours Can Transfer
ASHA allows CF transfers, and the hours you legitimately earned with a qualified mentor carry forward to your new site.1 The process works as follows:
Your current mentor must complete a CF Report and Rating Form documenting the hours and supervision you received during your time at the site.2
If you are mid-segment and have not yet reached 420 hours in that segment, you will need a supervision log detailing the direct and indirect supervision hours completed.2
Your new site's mentor assumes responsibility for the remaining hours and completes their own Report and Rating Form for subsequent segments.
All CF requirements, including the 36-week minimum and 1,260 total hours, still apply. The clock does not reset; it simply continues at your new placement.
The paperwork adds some administrative burden, but it is straightforward. The key is ensuring your outgoing mentor completes the required documentation before you leave.
Document Everything From Day One
If you suspect problems at your site, begin keeping written records immediately. This documentation serves multiple purposes: it protects you if hours are ever questioned, it provides evidence if you file a complaint, and it helps you articulate concerns to a prospective new employer.
Track the following:
Supervision logs: Record every direct and indirect supervision session, including date, duration, and topics covered. ASHA requires a minimum of 6 hours of direct supervision and 6 hours of indirect supervision per segment.2
Productivity demands: Save any written communications about caseload expectations, productivity percentages, or pressure to document services not provided.
Ethical concerns: Note specific incidents with dates, names, and what was said or done.
Even informal text messages or emails can become important records later.
Reporting Options When Problems Are Serious
If your site's issues rise to the level of ethical violations, you have formal recourse beyond simply leaving.
ASHA Board of Ethics: You can file a complaint using ASHA's required complaint form. The Board investigates alleged violations of the Code of Ethics, and possible outcomes range from dismissal of the complaint to reprimand, censure, probation, suspension, or revocation of ASHA membership and certification.3
State licensing boards: Each state has its own complaint process for licensed professionals. If your mentor is engaging in conduct that violates state practice standards, the licensing board can investigate independently of ASHA.2
Employment attorney: If you face retaliation for raising concerns, or if your contract includes provisions that seem designed to trap you, consulting an employment attorney can clarify your rights.
Reframing the Fear of Leaving
The fear of transferring is real but often overestimated. CFs worry about burning bridges, explaining a short tenure to future employers, or losing momentum. But consider the alternative: if your mentor is not providing the required supervision, those hours may not count anyway. If you are being pressured into unethical practices, your license and career are at risk before they even begin. Understanding the full scope of ASHA CF requirements can help you evaluate whether your site is meeting its obligations.
Post-start remedies remain the most under-discussed topic in CF planning. Most guidance focuses on choosing well upfront, which is important, but life does not always cooperate. Knowing that you have options, that your hours transfer, and that reporting mechanisms exist can give you the clarity to act when staying is the greater risk.
Common Questions About Clinical Fellowship Red Flags
Choosing a clinical fellowship site is one of the most consequential decisions you will make early in your career. The questions below address the concerns that come up most often among CFs navigating offers, contracts, and workplace culture. Each answer points back to a deeper discussion elsewhere in this guide.
What are red flags in a clinical fellowship setting?
Red flags include unrealistic productivity demands from day one, limited or absent direct supervision, pressure to bill for services that were not provided, high staff turnover, vague job descriptions, and restrictive contract clauses. Any single issue may be manageable, but a pattern of several together signals a site that prioritizes revenue over your professional growth. The severity framework earlier in this article can help you sort deal breakers from negotiable concerns.
What productivity percentage is reasonable for an SNF clinical fellowship?
Most experienced clinicians consider a starting productivity target between 75 and 85 percent reasonable for a new CF in a skilled nursing facility, with gradual increases as you build efficiency. A site that expects 90 percent or higher from the outset is placing billing quotas above clinical learning. The SNF-specific red flags section of this guide breaks down how to interpret the benchmarks a facility shares during your interview.
What ASHA supervision requirements must a CF site meet?
ASHA requires that your CF mentor hold the Certificate of Clinical Competence (CCC-SLP) and provide a minimum of 36 supervision activities over the fellowship period, including at least 18 direct observation sessions. On-site mentorship should be consistent and documented. If a prospective site cannot clearly explain how it meets these minimums, treat that as a significant red flag. Our supervision quality section offers a fuller checklist.
Are non-compete clauses common in clinical fellowship contracts?
Non-compete clauses do appear in some CF contracts, particularly those offered by staffing companies and large healthcare organizations. While they are not universal, their enforceability varies by state. A clause that restricts you from working within a broad geographic area or for an extended period after your fellowship ends deserves careful review, ideally by an attorney. The contract red flags section of this article details what to watch for.
What should I do if I discover red flags after starting my clinical fellowship?
Start by documenting specific concerns with dates and details. Raise issues with your CF mentor or site supervisor in writing when possible. If the problems involve supervision shortfalls or ethical violations, contact ASHA's Clinical Fellowship office for guidance on your options. Leaving a site mid-fellowship is not ideal, but it is far better than completing a fellowship under conditions that compromise your training or licensure.
How can I verify a CF mentor's qualifications before accepting an offer?
You can confirm that a prospective mentor holds current CCC-SLP certification through ASHA's online directory. Ask the mentor directly about their years of clinical experience, areas of specialization, and how many CFs they have supervised previously. Speaking with former fellows at the same site can also reveal whether mentorship is hands-on or largely absent. The mentorship quality section of this guide offers additional verification strategies.
Can I transfer my clinical fellowship to a different site if things go wrong?
Yes, ASHA allows you to transfer your clinical fellowship to a new site. The hours and supervision activities you have already completed in good standing can carry over, provided they are properly documented and your outgoing mentor submits the required paperwork. Transferring takes coordination, so reach out to ASHA early in the process. The section on discovering red flags after starting your CF walks through the practical steps involved.