Mastering Clinical Supervision in SLP Grad School: A Complete Guide
Practical strategies, feedback techniques, and documentation tools for building a strong supervision relationship in speech-language pathology.
By Benjamin Thompson, M.S., CCC‑SLPReviewed by SLP Editoral TeamUpdated July 17, 202625+ min read
Points of interest…
ASHA requires at least 25% direct observation during SLP graduate clinical hours.
Effective supervisors shift from directive to consultative feedback across 15 weeks.
Early documentation of performance concerns protects both students and supervisors.
Clinical supervision is often the single most powerful determinant of whether a graduate student leaves an SLP program with true clinical competence or merely a checklist of completed hours. Unlike coursework, which teaches theory and assessment protocols, supervision occurs in real time with real clients, where nuance, clinical judgment, and ethical decision-making are forged under the guidance of an experienced practitioner.
This article is written for two audiences: graduate students trying to understand what effective supervision should look like and how to advocate for their own learning, and supervisors who want practical strategies for structuring feedback, managing documentation, and navigating difficult conversations when a student's performance falls short.
The supervision relationship is distinct from every other academic or clinical pairing. It carries both formative and evaluative weight, blending mentorship with gatekeeping. A mismatch in expectations, unclear feedback loops, or poorly timed conflict can derail a semester or delay CCC-SLP certification.
What Is Clinical Supervision in Speech-Language Pathology?
What exactly does a clinical supervisor do in an SLP graduate program, and why does the role go so far beyond simply watching a student run a session?
More Than an Observer
Clinical supervision in speech-language pathology is a structured, mentoring relationship between a credentialed SLP and a student or early-career clinician during clinical practica. The supervisor is accountable not just for the supervisee's professional growth, but for the safety and quality of care received by every patient in the room. That dual accountability is what makes supervision distinct from coaching or informal feedback.
ASHA frames the purpose around three pillars: patient safety, competency development, and professional socialization. That last one often gets overlooked. Learning to think and behave like a clinician, to navigate uncertainty, to communicate with families and colleagues, is as much a part of graduate training as clocking direct contact hours.
Who Is Being Supervised?
Three distinct groups work under SLP supervision, and the rules differ for each.
Graduate students in accredited programs are completing the SLP clinical hours requirements for the Certificate of Clinical Competence (CCC-SLP), totaling 400 clock hours under current standards.1
Clinical Fellows (CFs) are fully graduated SLPs completing the post-degree mentored experience required before earning independent certification.
Speech-language pathology assistants (SLPAs) work under ongoing supervision throughout their careers, not as a transitional stage.
This article focuses primarily on graduate student supervision, though differences for CFs and SLPAs will come up later where they matter.
The Continuum of Supervision
ASHA's model describes supervision as a continuum, not a fixed level of oversight. Early in a practicum, supervision is more direct: the supervisor is present, observing closely, and stepping in when needed. As the student builds competence and confidence, supervision shifts toward a consultative mode, with the student taking greater initiative and the supervisor functioning more as a sounding board.
This scaffolding philosophy is intentional. Current standards require supervisors to provide direct supervision for at least 25% of a graduate student's total clinical contact time,2 and supervisors themselves must hold the CCC-SLP with at least nine months of professional experience.2 They are also required to complete two hours of professional development specifically in supervision.2
The approach is competency-based, meaning the goal is demonstrated skill, not seat time. That distinction shapes everything from giving constructive feedback to SLP students to how a supervisor decides when to step back and let the student lead.
Roles and Responsibilities: Supervisors Vs. Students
Clinical supervision in speech-language pathology works best when both parties understand where their responsibilities begin and end. Supervisors are not simply evaluators, and students are not passive observers. Both hold distinct but overlapping duties that shape the quality of the learning experience and, ultimately, the safety of client care.
What Supervisors Own
The supervising SLP carries responsibility for guidance, monitoring, and accountability.1 That includes providing instruction, modeling clinical decision-making, and giving feedback in a form the student can act on. Supervisors also maintain the professional standards a clinic or school placement requires: making sure documentation is accurate, sessions comply with facility policy, and the client's care is never compromised by a trainee's learning curve.2
Beyond compliance, supervisors are expected to monitor progress over time, not just session by session.3 Higher-education research on supervision relationships describes the role as part apprenticeship, part tutoring, and part partnership, with the supervisor offering intellectual and career support alongside structured clinical guidance.4 Regular contact, whether weekly meetings, mid-rotation check-ins, or informal debriefs after sessions, is part of the job.5
What Students Own
Graduate students are active participants, not recipients.1 They are responsible for completing assigned clinical work independently, following program rules, meeting training requirements, and engaging with the resources their program and site provide. That means preparing session plans on time, reviewing client files before treatment, and applying feedback rather than waiting for it to be repeated. Building confidence in SLP clinical placements takes exactly this kind of proactive preparation.
Students also carry a communication responsibility that is easy to overlook: raising problems early.2 If a caseload feels unsafe, a technique is unclear, or the supervisory relationship is strained, the student is expected to speak up before small issues become documented performance concerns.
Where the Roles Meet
One useful mindset: supervisors evaluate the work, students complete the work, and both share the relationship. Giving constructive feedback to SLP students is most effective when students are already fulfilling their side of this dynamic. When either side treats supervision as one-directional, the partnership breaks down.
Questions to Ask Yourself
Do you come to supervision meetings with specific clinical questions prepared, or do you typically wait for your supervisor to set the agenda?
Students who arrive with targeted questions often get more tailored guidance and use meeting time efficiently. Shifting from passive to active participation can accelerate skill development and demonstrate professional initiative.
When did you last ask a student directly what type of feedback helps them learn best?
Supervisors who check in about feedback preferences often discover that students need more modeling, written summaries, or real time cues. This simple question can prevent mismatched expectations and speed up clinical growth.
Are you documenting moments of uncertainty during sessions so you can discuss them later?
Jotting quick notes about confusing client responses or technique doubts gives supervision conversations concrete starting points. Without these specifics, meetings can drift toward general advice that may not address your actual gaps.
How comfortable are you giving upward feedback to your supervisor about what is or is not working?
Supervision is a two way relationship. Students who respectfully share what support they need help supervisors adjust their style, creating a more productive learning environment for everyone.
ASHA Supervision Requirements for SLP Grad Students
Supervision standards in speech-language pathology have grown more precise over the past decade, and understanding exactly what ASHA requires during graduate training can save both students and supervisors from costly compliance gaps.
The 25% Direct Supervision Rule
ASHA requires that graduate SLP students receive direct supervision for at least 25% of their total clinical contact hours.1 "Direct" means real-time oversight: the supervisor is physically present in the room or connected through live video. Reviewing a session recording after the fact does not count. Neither does reading session notes. The supervisor must be able to observe and, if necessary, intervene while the session is happening.
This standard applies across all SLP clinical placements during graduate training. If a student sees ten clients in a week, the supervisor must be directly observing during sessions that account for at least 25% of that total client contact time.
Who Qualifies as a Supervisor
Not every CCC-SLP can supervise a graduate student on day one. ASHA sets three baseline requirements:1
Credential: The supervisor must hold the CCC-SLP certification.
Experience: At least nine months of full post-certification practice must have passed before supervising.
Training: Completion of at least two hours of professional development specifically focused on supervision is required.
That two-hour training requirement is a meaningful quality check. It signals that ASHA views supervision as its own clinical skill, not an automatic extension of clinical competence.
Telesupervision: When Remote Counts
Synchronous, real-time video supervision qualifies as direct supervision under current ASHA policy.1 A supervisor observing a graduate student's session via live video feed, with two-way communication available, meets the standard. Asynchronous review, such as watching a recorded session the following day, does not.
Technology matters here. The connection must be stable enough to allow genuine real-time observation and immediate response. ASHA's guidance sets the functional standard; specific platform requirements may vary.
One important caveat: states regulate their own licensure, and some impose stricter telesupervision rules than ASHA does. A supervisor and student based in different states may face additional requirements from one or both licensing boards. Always cross-check with your SLP state licensing requirements before relying solely on ASHA's framework.
How Requirements Differ Across Roles
The 25% rule is specific to graduate students. Once someone enters the Clinical Fellowship, the model shifts. Clinical Fellows are not subject to a percentage-based supervision floor. Instead, their supervisors must complete at least six hours of direct observation and six hours of other mentoring activities per fellowship segment, totaling 18 hours of direct observation and 18 hours of mentoring across all three segments.1
SLPAs face a different and generally more restrictive framework. Because SLPAs practice under ongoing supervision rather than toward independent licensure, ASHA recommends at least 50% direct supervision when working with students in school settings, and up to 100% direct supervision when clients have complex medical needs.2 SLPAs do not move toward independent practice: supervision is a permanent structural feature of the role, not a transitional phase.
All three populations, graduate students, Clinical Fellows, and SLPAs, require supervisors who hold the CCC-SLP, have at least nine months of post-certification experience, and have completed the two-hour supervision training.1 The credential baseline is consistent; the intensity and structure of what supervision looks like in practice varies considerably by role.
A Practical Reminder About State Law
ASHA's standards represent a national floor, not a ceiling. States frequently layer additional requirements on top: higher direct supervision percentages, mandatory supervision logs in specific formats, or restrictions on which settings qualify for telesupervision. Before finalizing any supervision arrangement, both the supervisor and the student should verify current requirements with their state licensing board. What satisfies ASHA's certification standards may not fully satisfy state licensure law, and it is the state license that ultimately determines whether a graduate can practice after completing their degree.
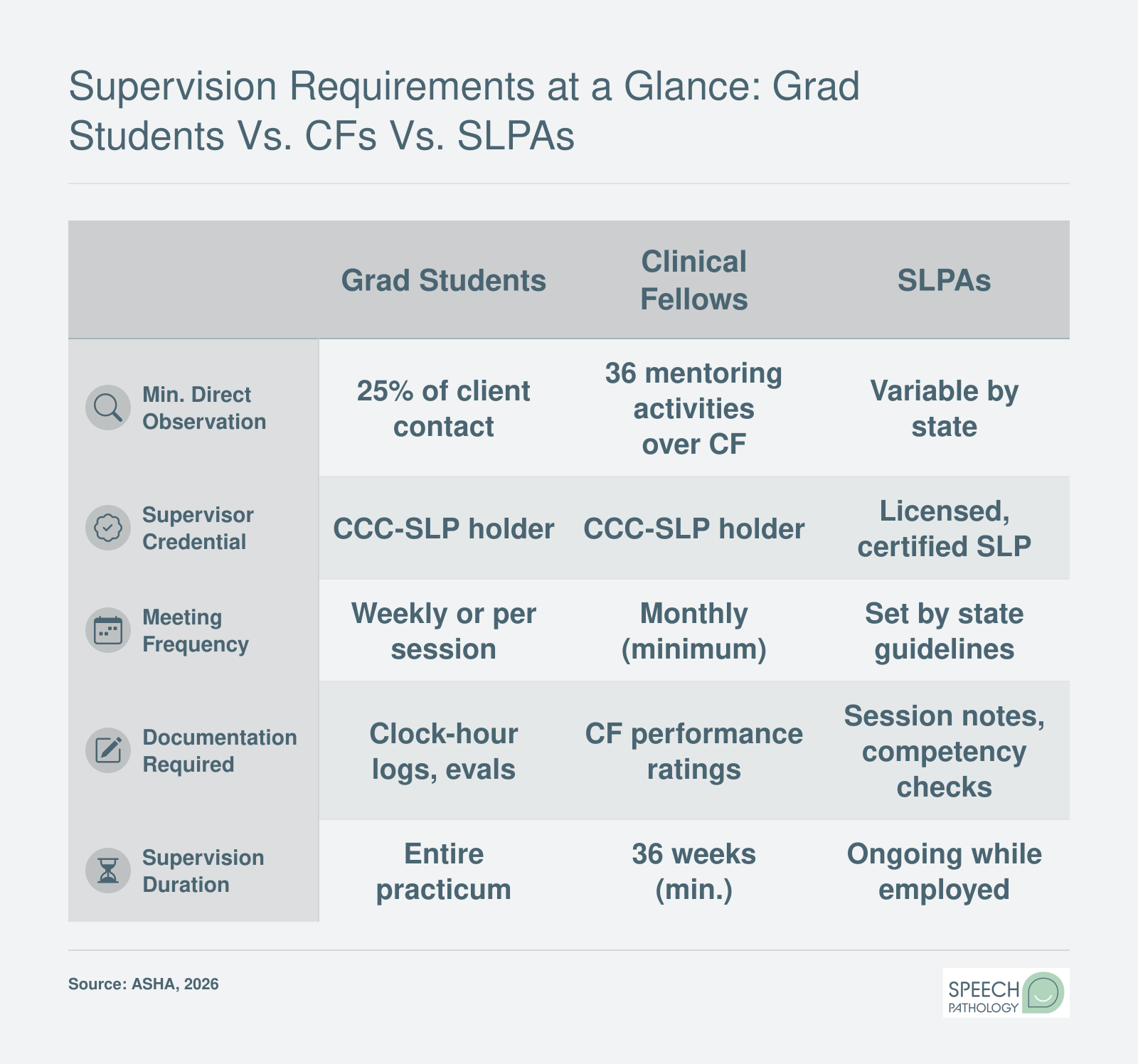
Supervision Requirements at a Glance: Grad Students Vs. CFs Vs. SLPAs
ASHA sets distinct supervision standards depending on where a clinician falls on the professional development continuum. This side-by-side comparison highlights the key differences in observation time, supervisor qualifications, meeting frequency, and documentation expectations across the three supervisee categories.
Effective Feedback Strategies for SLP Supervisors
In a 2021 survey of clinical supervision practices, 64 percent of SLP supervisors reported using corrective feedback as their primary formative tool, yet only 27 percent consistently set agendas for supervision sessions.1 This gap highlights a common challenge: supervisors often focus on what students did wrong without establishing structured frameworks that teach students how to self-assess and problem-solve. Effective clinical feedback in speech-language pathology requires more than pointing out errors. It demands intentional models, strategic questioning, and balanced delivery that builds clinical competence and reflective thinking.
Evidence-Based Feedback Models for SLP Supervision
Three frameworks stand out in clinical education research. Anderson's Continuum of Supervision moves students through three stages: evaluation-feedback (supervisor-driven assessment), transitional (collaborative problem-solving), and self-supervision (student-led reflection).2 The model encourages supervisors to gradually release control as students demonstrate growing clinical judgment. ASHA's Supervision Quality Framework (SQF) identifies three feedback types: confirming (reinforcing effective behaviors), corrective (addressing errors), and guiding (prompting reflection before a decision point).2 Finally, the R2C2 Model structures post-session conversations around four steps: building rapport, eliciting the student's reactions, reviewing content together, and coaching for change.3 Research shows that effective feedback delivers one to three key points per task, is based on direct observation, and remains descriptive rather than evaluative.3
Concrete Feedback Script Examples
Phrasing matters. During a session, a supervisor might redirect in real time by saying, "I notice the child is losing focus. What strategy could you try right now to re-engage him?" This prompts immediate problem-solving without derailing the session. After a session, a debrief might begin with, "Walk me through your decision to skip the auditory bombardment step. What were you noticing in the moment?" This invites the student to articulate clinical reasoning rather than passively receive critique. When addressing a recurring pattern, a supervisor could say, "I've observed that you tend to provide the correct answer when a client struggles. Let's brainstorm three cueing strategies you can use instead during our next session." This frames the issue as a skill to build, not a deficiency to criticize. For a deeper look at structuring these conversations, giving constructive feedback to SLP students offers additional scripts and practical guidance.
Strategic Questioning for Reflective Practice
Open-ended questions shift students from dependence to independence. Instead of "You should have used a visual schedule," ask "What would you change if you ran that session again?" This question transfers ownership of the solution. "How did you decide which cues to use with that client?" prompts students to articulate their clinical decision-making process. "What data will help you determine if this goal is appropriate?" teaches students to ground clinical choices in evidence-based practice in speech-language pathology. These questions mirror the reflective thinking students will need as independent clinicians.
Balancing Positive and Constructive Feedback
The traditional "praise-criticism-praise" sandwich often feels formulaic and undermines trust. Research in clinical supervision recommends specific, behavior-linked praise instead.2 Rather than "Good job today," try "You adjusted your pacing when the client seemed overwhelmed. That showed strong clinical flexibility." This ties praise to observable actions and reinforces the reasoning behind effective choices. When offering corrective feedback, use I-statements and keep it descriptive: "I observed three instances where the client self-corrected, but those weren't documented. Let's review how to capture that data in real time."2 Discussing feedback preferences upfront during initial supervision meetings helps tailor delivery to each student's learning style and builds rapport before corrective conversations arise.4
Did You Know?
The hallmark of great SLP supervision is moving from an early directive stance, where clear instructions are vital, to a later consultative role that invites student reflection and decision-making. Without this shift, graduates may perform tasks correctly but fail to develop the autonomous, critical-thinking skills essential for treating diverse clients. This progression is what separates true clinical educators from simple instructors.
How to Structure a Semester-Long Supervision Plan
What does a well-paced 15-week supervision plan actually look like from week one to the final evaluation? The answer is a phased structure that gradually transfers clinical responsibility from supervisor to student, with clear checkpoints along the way.
Phase 1: Orientation and Observation (Weeks 1-3)
The opening weeks establish safety, expectations, and baseline skills. Plan for 100% direct observation during any student-led contact, with the supervisor modeling sessions for the first week and co-treating in weeks two and three.
Feedback cadence: daily debriefs of 10-15 minutes after each session, plus one 45-minute weekly conference to review goals and paperwork.
Student deliverables: a written learning contract, two self-identified growth goals, observation notes on three supervisor-led sessions, and a first attempt at a SOAP note for co-signature.
Checkpoint: end of week 3, the supervisor confirms the student is ready to lead sessions independently on a limited caseload.
Phase 2: Guided Independence (Weeks 4-10)
This is the longest and most instructionally dense phase. Direct observation drops to roughly 50-75% of sessions, with the supervisor rotating across the caseload rather than watching every contact.
Feedback cadence: brief daily debriefs continue, and weekly conferences expand to include video review of one recorded session.
Student deliverables: independent lesson plans, weekly self-evaluations tied to the ASHA Big 9, two full video-review assignments, and progress notes written without prompting.
Checkpoints: a mid-placement formative evaluation at week 7 using the program's competency rubric, and a caseload expansion trigger once the student demonstrates independent planning and safe clinical judgment on the starter caseload.
Phase 3: Independent Practice with Consultative Supervision (Weeks 11-15)
Direct observation drops to the ASHA minimum of 25% for graduate practicum, and the supervisor shifts into a consultative role. The student manages the daily schedule, family communication, and documentation with spot-check oversight.
Feedback cadence: debriefs move to as-needed, and weekly conferences focus on caseload management and professional identity.
Student deliverables: a capstone case study, a self-directed remediation plan for any lagging competencies, and a summative self-evaluation submitted before the final review.
Checkpoint: end-of-placement summative evaluation against program benchmarks.
Calibrating for Setting and Skill Level
School placements often front-load observation because of IEP timelines and mandated reporter responsibilities. Hospital and SNF settings usually require longer orientation for infection control, chart access, and interdisciplinary rounds, so Phase 1 may stretch to four weeks. Private practice placements can move faster on session independence but slower on billing and documentation. Understanding the demands of each environment is easier when you can compare SLP career settings side by side.
For a first placement, weight the timeline toward Phase 2. For a final SLP externship, compress Phase 1 to a single week and expand Phase 3 so the student leaves ready for the Clinical Fellowship. Knowing what a typical day looks like for an SLP graduate student can also help supervisors set realistic phase expectations from the start.
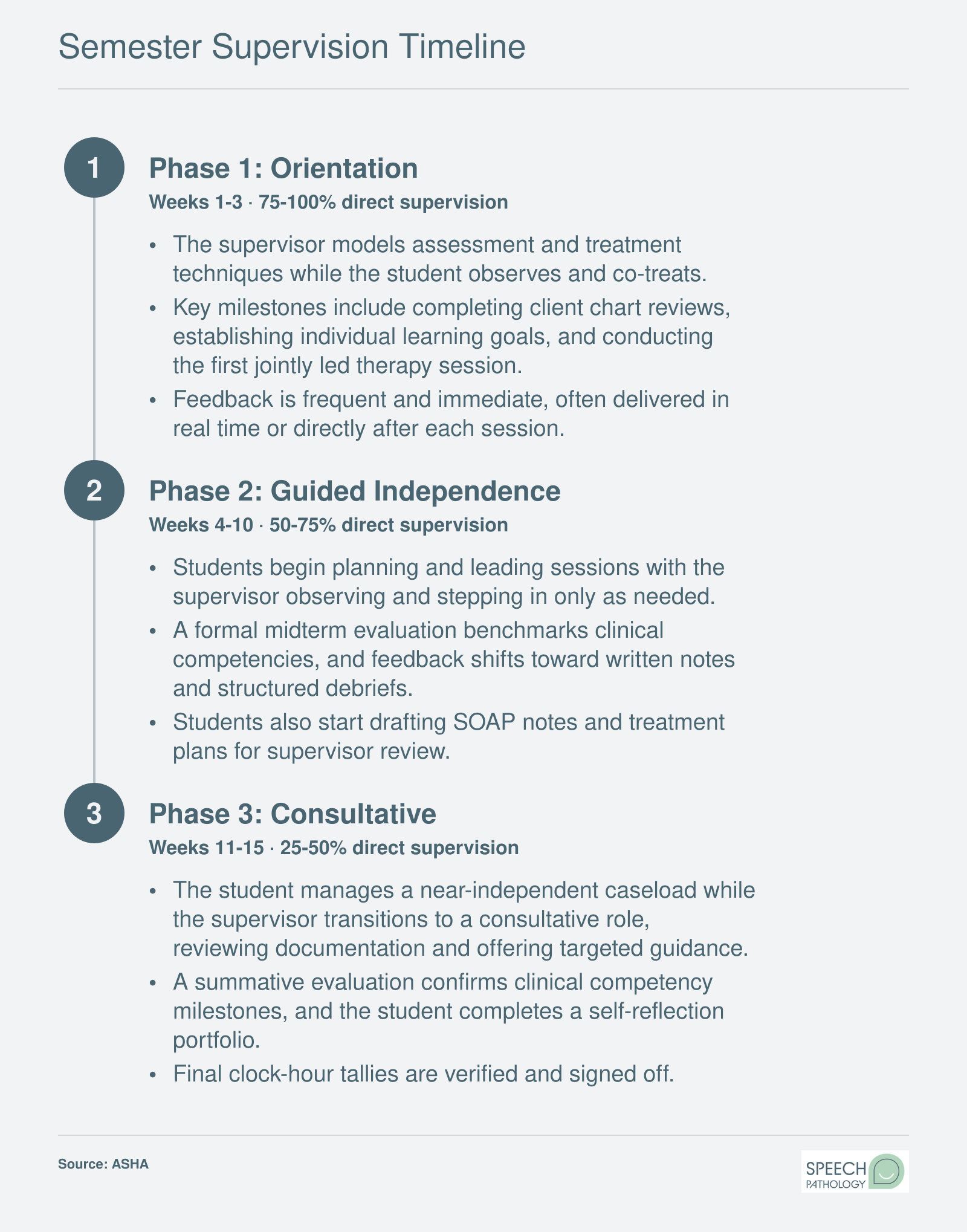
Semester Supervision Timeline
A typical 15-week clinical practicum follows three supervision phases, each designed to gradually shift responsibility from the supervisor to the student. Here is how the semester unfolds, including the recommended minimum observation percentages set by ASHA at each stage.
SLP Supervision Documentation Templates and Tools
Supervision documentation is the paper trail that connects every clinical interaction, feedback conversation, and skill milestone throughout your graduate program. When done well, it keeps both supervisors and students aligned on expectations, satisfies ASHA compliance requirements, and provides a safety net if disagreements or remediation concerns arise later. Below are the core documents every supervision relationship should maintain, along with digital tools that make the process more manageable.
Five Essential Documents
A well-organized supervision file typically includes the following:
Supervision contract or agreement: This document establishes the ground rules before clinical work begins. It should outline each party's responsibilities, meeting frequency, preferred feedback methods, confidentiality expectations, and procedures for conflict resolution. Many university programs require a signed contract at the start of each practicum rotation.
Direct-observation log: Supervisors must document every session they observe, including the date, duration, setting, client information, and specific skills assessed. Programs like the one at Idaho State University require fields such as guided observation hours, the university name, and the supervisor's ASHA number to ensure accurate recordkeeping.1
Feedback session notes: After each supervisory conference, a brief written summary captures what was discussed, goals set for the next session, and any action items. Best practice guidance suggests completing these notes within 24 hours while details are still fresh.2
Mid-term and final evaluation forms: Structured evaluations, often built around ASHA's Knowledge and Skills Acquisition (KASA) competencies or their updated equivalents, give students a formal snapshot of their progress. These forms also create a documented basis for grading decisions and, if needed, remediation planning.
Clinical hours tracking sheet: Every direct and indirect clinical contact hour must be logged accurately. This running tally feeds into the total hours students need for graduation and eventual certification.
A comprehensive supervision file may also include development plans, remediation records, relevant correspondence, and copies of any client disclosure forms related to student involvement in care.3 ASHA's health care documentation standards further specify that all records be signed and dated, with clinician credentials noted and any student, clinical fellow, or assistant participation clearly identified.4
Digital Platforms Worth Knowing
Several platforms help supervisors and students manage documentation electronically rather than juggling spreadsheets and paper folders.
CALIPSO: Widely adopted by graduate programs across the country, CALIPSO allows students to log clinical hours, supervisors to complete evaluations online, and program directors to monitor compliance in real time. Its main strength is standardization; its main drawback is that access typically requires a program-level subscription, so individual users cannot purchase it independently.
Typhon: Common in health science programs beyond SLP, Typhon offers robust tracking for clinical hours, patient encounters, and supervisor evaluations. It tends to be feature-rich but can feel complex for users who only need basic hour logging.
Custom Google Forms or spreadsheet trackers: Some programs and individual supervisors build their own tracking systems using Google Forms linked to shared spreadsheets. These are free and highly customizable, but they lack the built-in validation and reporting features of dedicated platforms, which can lead to data entry errors or inconsistencies over time.
Why Documentation Protects Both Parties
Think of supervision documentation as a shared record of truth. If a student's clinical performance raises concerns midway through a semester, supervisors who have consistently documented feedback and observation notes can demonstrate that issues were identified early and addressed transparently. For practical strategies on delivering that feedback effectively, see our guide on giving constructive feedback to SLP students. Students benefit equally: clear records show the support and guidance they received, which matters if they need to appeal a grade or dispute a remediation decision.
Documentation is not busywork. It is the backbone of accountability in clinical education, and understanding what a typical day looks like for an SLP graduate student can help you see how these documentation habits fit into the broader rhythms of grad school, carrying you well through your clinical fellowship and beyond.
Navigating Conflict and Remediation in SLP Supervision
Conflict and performance concerns are inevitable in clinical training, and addressing them early with clear expectations and documentation protects both students and supervisors. When a graduate student struggles to meet competency benchmarks or interpersonal friction arises between supervisor and supervisee, a structured remediation process ensures fairness, accountability, and an opportunity for growth.
Recognizing When Remediation Is Needed
Supervisors should intervene when a student consistently demonstrates gaps in clinical skills, professionalism, ethical judgment, or the ability to accept feedback. Common triggers include repeated lapses in safety protocols, inability to modify treatment plans despite coaching, unresolved attendance or punctuality issues, or patterns of defensive or dismissive responses during supervision conferences. Early identification allows for corrective action before problems compound or jeopardize patient care.
Many university SLP programs publish remediation policies and templates in their clinical education handbooks or departmental resources. Searching for terms like "remediation plan" or "remediation policy" on program websites can yield sample forms and timelines that outline required meetings, documentation intervals, and criteria for successful completion or dismissal from clinical placements.
Building a Fair Remediation Plan
An effective remediation plan includes specific, measurable goals with clear deadlines. Rather than stating "improve clinical skills," a plan might require the student to independently complete three consecutive dysphagia evaluations with 90 percent accuracy on a supervisor-approved checklist by the end of a four-week period. The plan should also name the support resources available, such as additional observation hours, peer mentoring, or targeted readings, and specify the consequences if benchmarks are not met.
ASHA's website offers resources on constructive feedback for SLP students, including the "Clinical Supervision in Speech-Language Pathology" document and ethical decision-making frameworks like the "ASHA Code of Ethics" and "Issues in Ethics" statements. These materials help supervisors distinguish between performance issues that warrant remediation and conduct violations that may require immediate escalation to program directors or ethics committees.
Conflict Resolution and Communication
Not all supervision challenges stem from skill deficits. Personality clashes, cultural differences in communication style, or mismatched expectations about autonomy can create friction. When conflict arises, supervisors should request a neutral third party, such as a clinical coordinator or faculty advisor, to facilitate a conversation focused on observable behaviors rather than character judgments. Documenting these discussions protects all parties and ensures continuity if the student rotates to a new supervisor mid-semester.
The Council on Academic Accreditation standards and ASHA Learning Pass courses on managing underperforming students provide actionable strategies for de-escalation, progressive feedback, and legal compliance. Students who are weighing whether to continue in a program after a difficult remediation experience may find guidance in resources on transferring SLP graduate programs. State licensing boards may also offer general workplace conflict resolution guidelines, though SLP-specific remediation frameworks are most often housed within university programs and national professional organizations.
Did You Know?
Supervisors: if you notice a performance concern, address it early and document that conversation. Research and experienced clinicians consistently show that students who receive timely, specific feedback can correct course effectively, while waiting until a final evaluation often leaves students feeling blindsided and limits their ability to improve.
Career Outlook for SLPs and Clinical Educators
Understanding compensation and job growth can help you weigh whether to stay in direct clinical practice or move into a clinical education role. The Bureau of Labor Statistics projects 15% job growth for speech-language pathologists from 2024 to 2034, translating to roughly 28,200 new positions and about 13,300 annual openings nationwide. Below is a side-by-side look at national wage data for practicing SLPs and postsecondary health specialties teachers, a category that includes many clinical supervisors and faculty members in SLP programs.
Role
Total National Employment
25th Percentile Salary
Median Salary
Mean Salary
75th Percentile Salary
Speech-Language Pathologists
178,790
$75,310
$95,410
$95,840
$112,510
Health Specialties Teachers, Postsecondary
229,720
$74,400
$105,620
$137,900
$176,090
Frequently Asked Questions About SLP Clinical Supervision
Clinical supervision is one of the most important parts of your graduate training in speech-language pathology, and it naturally raises a lot of questions. Below are answers to the most common questions from both students and supervisors, drawn from ASHA guidelines and best practices covered throughout this guide.
What are the ASHA requirements for supervising SLP graduate students?
ASHA requires that clinical supervisors hold the Certificate of Clinical Competence in Speech-Language Pathology (CCC-SLP) and have completed a minimum of nine months of post-certification clinical experience. Supervisors must also complete at least two hours of professional development in clinical supervision. These requirements help ensure that supervisors have both the clinical expertise and the instructional skills to guide graduate students effectively through their practicum experiences. For a closer look at what CCC-SLP certification requires, including timelines and costs, see our full certification guide.
How much direct supervision is required for SLP grad students?
ASHA mandates that graduate students receive direct supervision for at least 25% of each client or patient contact during their clinical practicum. In many programs, the percentage starts significantly higher, sometimes at 50% or more, during a student's first clinical placement and then gradually decreases as the student demonstrates increased competence. Direct supervision means the supervisor is physically present and observing the session in real time.
What is the difference between supervising SLP grad students, CFs, and SLPAs?
The key differences relate to the level of independence and the supervision intensity required. Graduate students need the highest level of direct observation (at least 25% of contact time), while Clinical Fellows require a minimum of 36 mentoring activities across 36 weeks with direct observation of at least 6 hours. Our ASHA Clinical Fellowship guide covers CF mentoring requirements in full detail. SLPAs, on the other hand, must receive ongoing supervision that includes at least 10% direct and 10% indirect supervision of their total work time on a weekly basis. Students who are working as an SLPA in grad school should pay particular attention to how these supervision ratios apply to their own role.
How should SLP supervisors give constructive feedback?
Effective feedback in SLP supervision is specific, timely, and balanced. Supervisors should reference observable behaviors rather than making general statements, and they should pair areas for growth with recognition of strengths. Using a structured framework, such as asking the student for self-reflection before offering your observations, encourages critical thinking. Written and verbal feedback should be combined, and feedback sessions should be scheduled regularly rather than reserved only for moments when problems arise.
What documentation is needed for SLP clinical supervision?
Supervisors should maintain records that include clock hour logs showing direct client contact time, documentation of supervisory meetings with dates and topics discussed, written feedback and evaluation forms, and remediation or action plans if applicable. Students are also responsible for tracking their own hours and securing supervisor signatures. Using standardized templates helps keep documentation organized and ensures compliance with both university and ASHA record-keeping standards.
How can SLP grad students get the most out of clinical supervision?
Students benefit most when they come to each supervision meeting prepared with specific questions, completed session notes, and honest self-reflections on what went well and what felt challenging. Setting personal clinical goals at the start of each practicum rotation gives supervision sessions a clear focus. Being open to feedback, asking for clarification when needed, and actively applying suggestions in the next session are habits that accelerate clinical growth and strengthen the student-supervisor relationship. For a broader picture of how supervision fits into your daily routine, see our look at a typical day for an SLP graduate student.