The Complete Guide to SLP Assessment Tools & Evaluation Resources
Compare standardized tests, free tools, and informal methods across every speech-language disorder area — with age ranges, admin times, and selection tips.
By Benjamin Thompson, M.S., CCC‑SLPReviewed by SLP Editoral TeamUpdated August 4, 202625+ min read
Points of interest…
SLPs organize standardized assessment tools by disorder area, covering articulation, language, fluency, voice, and swallowing.
Dynamic and informal methods like language sampling prevent overreliance on any single norm-referenced test.
Applying English-only norms to bilingual children can inflate overidentification rates by two to three times.
Free resources and telehealth-adapted tools are expanding access to quality evaluations in school and clinical settings.
Every eligibility decision, IEP goal, and treatment plan an SLP writes begins with assessment. ASHA's 2023 Schools Survey found that school-based clinicians spend roughly 20 percent of their weekly hours on evaluation activities, yet many report feeling undertrained in selecting and interpreting the right instruments. The challenge is real: the field offers hundreds of options spanning standardized norm-referenced tests, informal checklists, dynamic assessment protocols, free screening tools, and bilingual measures, each with distinct psychometric properties and population constraints.
Choosing the right tool matters as much as administering it correctly. A mismatch between instrument and client can inflate error rates, delay services, or produce goals disconnected from functional need. As telepractice speech therapy expands and caseloads grow more linguistically diverse heading into 2026, the selection process is only getting more complex. This guide walks you through standardized tools organized by disorder area, informal and dynamic assessment methods, free resources, bilingual evaluation considerations, telehealth adaptations, and a step-by-step evaluation workflow so you can approach every assessment with confidence.
What Are SLP Assessment Tools and Why Do They Matter?
SLP assessment tools encompass any instrument or procedure a speech-language pathologist uses to measure a client's communication, swallowing, or cognitive-linguistic abilities. That definition is deliberately broad. An assessment tool might be a commercially published test kit with scoring manuals, a structured language sample protocol, a parent questionnaire, a bedside swallow screen, or a real-time observation checklist. Understanding what these tools are, and why they carry so much weight in clinical decision-making, is the first step toward building a well-rounded evaluation skill set.
Three Core Purposes of Assessment
Every assessment an SLP conducts serves at least one of three goals:
Eligibility determination: Does this individual qualify for services under a medical diagnosis, insurance criteria, or educational classification? Accurate assessment data drives that decision.
Baseline measurement and treatment planning: Before therapy begins, clinicians need a clear picture of current abilities so they can set measurable goals and choose evidence-based interventions.
Progress monitoring and discharge decisions: Ongoing assessment tells clinicians whether a client is improving, plateauing, or regressing, and it supports the clinical judgment to modify, continue, or end services.
These three purposes recur across every work setting, from schools and hospitals to private practices and early intervention programs. If you are still exploring the broader landscape of the profession, our guide on how to become a speech-language pathologist covers the educational and certification requirements that lead to clinical practice.
Two Big Categories: Formal vs. Informal
Throughout this guide you will see assessment tools sorted into two overarching categories:
Formal (standardized, norm-referenced) tools: These are published tests administered and scored according to strict protocols. They compare an individual's performance to a normative sample and yield standard scores, percentile ranks, or age equivalents.
Informal (criterion-referenced, observational, dynamic) tools: These include language samples, interviews, checklists, curriculum-based measures, and dynamic assessment procedures. They describe what a client can or cannot do without relying on a normative comparison group.
Both categories play essential roles. The American Speech-Language-Hearing Association's scope of practice makes clear that a comprehensive evaluation should draw on multiple sources of information. No single test, no matter how well-normed, is sufficient on its own to capture the full picture of a client's communicative functioning. For a deeper look at how these tools fit into the broader clinical workflow, see our SLP Evaluation & Treatment Planning Guide.
Why Tool Selection Carries Legal Weight
In school-based settings, the stakes extend beyond clinical best practice into federal law. The Individuals with Disabilities Education Act (IDEA) mandates that evaluations be nondiscriminatory, conducted in the child's dominant language whenever feasible, and multifaceted. That means relying on a single standardized test to determine eligibility is not just poor practice; it can violate a student's legal rights. SLPs must select, administer, and interpret a combination of tools that together provide a fair and thorough picture of the child's abilities.
Whether you are a graduate student preparing for your first clinical placement or a practicing clinician expanding your assessment toolkit, understanding these foundational categories and purposes will help you navigate the detailed tool reviews and selection strategies covered in the sections ahead.
Standardized Assessment Tools by Disorder Area
Standardized assessments give SLPs a norm-referenced framework for measuring a client's abilities against age-matched peers. Because no single test covers every communication domain, clinicians typically maintain a toolkit organized by disorder area. The table-style guide below groups the most widely used instruments by clinical focus, listing the publisher, intended age range, approximate administration time, and approximate kit cost.
A quick note before you dive in: the costs shown are publisher list prices for complete kits as of the 2025-2026 catalog cycle and are subject to change. Prices may differ when purchased through authorized resellers, and supplemental record forms are almost always an additional recurring expense. Always confirm current pricing directly with the publisher before budgeting.
Articulation and Phonology
The Goldman-Fristoe Test of Articulation, Third Edition (GFTA-3) remains the go-to choice for evaluating speech-sound production across clinical and school settings.1
GFTA-3: Published by Pearson Clinical. Designed for ages 2 through 21. Administration takes roughly 5 to 10 minutes, making it one of the quickest standardized tools in common use. Complete kit pricing typically falls between $420 and $480.1
Clinicians who need a deeper phonological-process analysis often pair the GFTA-3 with the Khan-Lewis Phonological Analysis, Third Edition, which uses the same speech sample.
Receptive and Expressive Language
Language assessments tend to command the largest share of an SLP's evaluation budget because they cover broad age ranges and multiple subtests.
CELF-5 (Clinical Evaluation of Language Fundamentals, Fifth Edition): Published by Pearson Clinical. Covers ages 5 through 21. Allow 30 to 45 minutes for core subtests. Kit pricing ranges from approximately $1,050 to $1,200, reflecting the depth of the test battery.2
PLS-5 (Preschool Language Scales, Fifth Edition): Published by Pearson Clinical. Targets birth through age 7, making it a staple in early-intervention programs. Administration runs about 20 to 30 minutes. Expect to pay between $520 and $580 for the complete kit.3
TOLD-P:5 (Test of Language Development, Primary, Fifth Edition): Published by Pro-Ed and distributed through WPS. Normed for ages 4 through 8. Takes roughly 20 to 30 minutes to administer, with kit pricing around $320 to $350.4
OWLS-II (Oral and Written Language Scales, Second Edition): Published by PAR, Inc. Spans ages 3 through 21 and uniquely measures listening comprehension, oral expression, and reading comprehension in a single instrument. Administration time averages 20 to 30 minutes per scale, and the full kit runs approximately $860 to $900.5
The CELF-5 is widely regarded as the gold standard for school-age language assessment, though it carries the highest price tag. For preschool populations, the PLS-5 offers comparable clinical depth at a lower cost.
Fluency
Fluency evaluations rely on a smaller pool of standardized instruments, with one clear frontrunner.
SSI-4 (Stuttering Severity Instrument, Fourth Edition): Published by Pro-Ed. Normed for ages 2 through 18 (with adult extensions available for clinical use). The assessment takes about 5 to 15 minutes and is one of the most affordable standardized tools at roughly $180 to $220.4
The SSI-4 quantifies stuttering frequency, duration, and physical concomitants into a single severity rating, which makes it valuable for establishing baselines and tracking progress over time.
Voice
Voice assessment leans heavily on instrumental measures and clinician-rated perceptual scales. The Consensus Auditory-Perceptual Evaluation of Voice (CAPE-V) is freely available from ASHA and is widely used alongside acoustic analysis software. Patient self-report instruments such as the Voice Handicap Index (VHI) supplement clinical observations and help document the functional impact of a voice disorder.
Feeding and Swallowing
Swallowing assessments are primarily instrumental rather than paper-and-pencil tests. The Modified Barium Swallow Study (MBSS) and Fiberoptic Endoscopic Evaluation of Swallowing (FEES) are the two cornerstone procedures. Costs for these evaluations are facility-dependent, covering equipment, supplies, and radiology or endoscopy fees rather than a single kit price. SLPs working in acute care vs inpatient rehab speech pathology settings will encounter these instrumental protocols most frequently, while clinicians often pair instrumental results with bedside screening tools to form a complete clinical picture.
Choosing Across Disorder Areas
When you are building or expanding your assessment library, start with the tools that align with your primary caseload. A school-based SLP might prioritize the GFTA-3 and CELF-5, while a pediatric speech language pathologist may lean toward the PLS-5 and TOLD-P:5 for younger populations. Regardless of setting, pairing standardized tools with informal and dynamic assessment methods, covered in the next section, leads to the most well-rounded evaluation.
Questions to Ask Yourself
When was the last time you paired a standardized test with a language sample or dynamic assessment?
Standardized scores alone can miss functional communication strengths and weaknesses. Combining formal results with a language sample or dynamic assessment gives you a fuller picture and strengthens your clinical recommendations.
Do your current go-to tools adequately represent the linguistic and cultural backgrounds of your caseload?
Many widely used standardized tests were normed on predominantly monolingual English speakers. If your caseload includes bilingual or culturally diverse clients, results from those tools alone may lead to over- or under-identification of disorders.
Are you selecting assessments based on habit, or based on the specific referral question?
Defaulting to the same battery for every client saves time but may not target the skill areas in question. Aligning each tool to the referral concern improves diagnostic accuracy and keeps evaluation sessions efficient.
Have you recently reviewed the technical manuals of the tests you use most often?
Normative data, reliability coefficients, and validity evidence can shift with updated editions. Staying current on your instruments' psychometric properties helps you interpret scores responsibly and defend your findings in eligibility meetings.
Informal and Dynamic Assessment Methods SLPs Should Know
Standardized tests are only one piece of the puzzle. Informal and dynamic assessment methods give speech-language pathologists a window into how clients actually communicate in real-world contexts, and ASHA makes it clear that these tools are not lesser alternatives. They capture functional communication skills that norm-referenced instruments often miss, making them essential for a well-rounded evaluation.
Language Sample Analysis: The Gold-Standard Informal Tool
Language sample analysis (LSA) is widely considered the most powerful informal measure available to SLPs. By recording and transcribing a client's spontaneous speech during conversation, narration, or play, clinicians can calculate key metrics that reveal a great deal about language development and use:
Mean Length of Utterance (MLU): Measures average utterance length in morphemes, offering a snapshot of grammatical complexity.
Type-Token Ratio (TTR): Compares the number of unique words to total words, providing insight into vocabulary diversity.
Narrative analysis: Evaluates story grammar elements such as setting, problem, and resolution to assess higher-level language organization.
Two free software tools make LSA accessible to clinicians and students alike. SALT (Systematic Analysis of Language Transcripts) offers a free educational version, while CLAN (Computerized Language Analysis) is freely available through the CHILDES database. Both automate many of the calculations that would otherwise take hours by hand.
Dynamic Assessment: Differentiating Difference from Disorder
Dynamic assessment follows a test-teach-retest framework. The clinician first evaluates a skill, provides targeted instruction or mediated learning, and then re-evaluates to measure how much the client improved with support. This approach, grounded in the framework developed by Lidz and Peña, is particularly valuable when working with bilingual speech pathologist caseloads and culturally diverse populations because it separates true language disorders from language differences rooted in varied linguistic experience. A child who responds quickly to brief instruction (high "modifiability") is more likely experiencing a language difference rather than a disorder. For more tools that support multilingual evaluation, explore our bilingual SLP resources.
Other Informal Methods Worth Knowing
SLPs draw on a range of additional informal strategies depending on the client and setting:
Behavioral observation: Watching how a client communicates during unstructured activities reveals pragmatic skills, turn-taking patterns, and compensatory strategies.
Criterion-referenced checklists: These tools measure performance against specific skill benchmarks rather than age-based norms, making them useful for tracking progress over time.
Play-based and analog tasks: Particularly effective with young children, these tasks elicit natural communication through toys, games, or role-play scenarios.
Curriculum-based measures: In school settings, SLPs can assess a student's language skills using actual classroom materials, connecting evaluation results directly to educational goals.
A Practical Tip for Comprehensive Evaluations
A defensible evaluation report pairs at least one formal and one informal measure for each domain assessed. For example, if you administer a standardized receptive language test, supplement it with a language sample analysis targeting the same skill area. This combination gives you both norm-referenced data for eligibility decisions and functional evidence that guides meaningful therapy goals. Supervisors, school teams, and insurance reviewers are far more likely to support your recommendations when they see converging evidence from multiple assessment types.
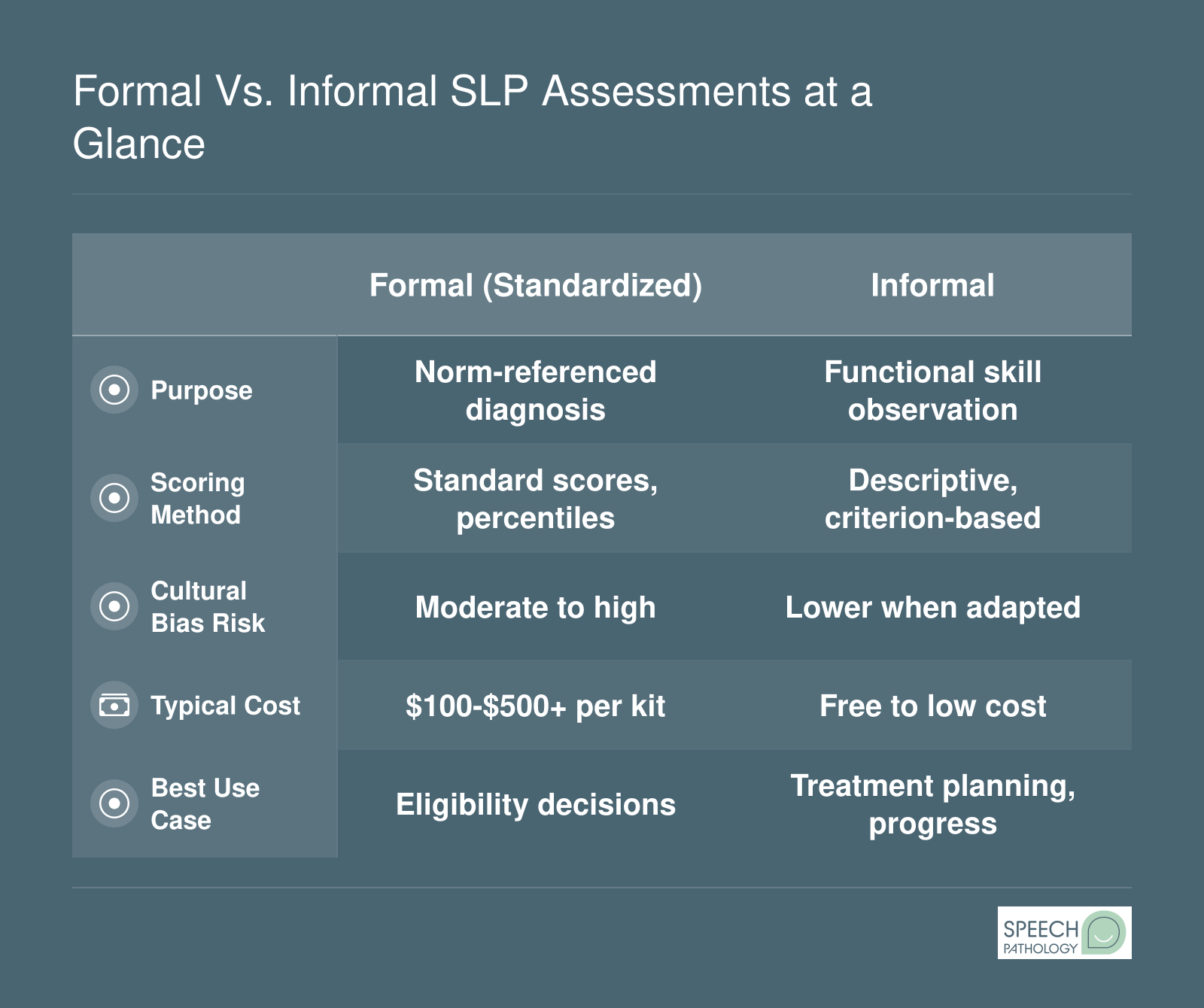
Formal Vs. Informal SLP Assessments at a Glance
Speech-language pathologists rely on both formal and informal assessments to build a complete clinical picture. Understanding how these two approaches differ across key attributes helps you choose the right tool for each client and setting.
Free and Low-Cost SLP Assessment Resources
Budget constraints are a reality in most clinical and school settings, but a growing number of free and low-cost tools can help speech-language pathologists gather meaningful data without stretching limited funds. Knowing which resources are available, and understanding their appropriate scope, puts you in a stronger position whether you are a graduate student building a clinical toolkit or a working SLP supplementing your test library.
Free Screening and Assessment Instruments
Several well-validated screening tools are available at no cost, each targeting a different area of practice.
SLUMS (Saint Louis University Mental Status Examination): A brief cognitive screening measure available from Saint Louis University's website. It is widely used with adults in medical settings and offers scoring adjustments for education level.
VHI (Voice Handicap Index): A 30-item self-report questionnaire that quantifies a client's perceived voice difficulty. The original VHI is published in peer-reviewed literature and can be reproduced for clinical use.
EAT-10 (Eating Assessment Tool): A 10-item swallowing screening questionnaire that helps identify individuals who may need a comprehensive dysphagia evaluation. It is freely available through its original publication.
ASQ (Ages and Stages Questionnaires): While the full ASQ system requires a license, many state early intervention programs provide free parent-completed screening forms based on ASQ norms. Check your state's Part C program website for downloadable versions.
CSBS-DP Infant-Toddler Checklist: Developed by Amy Wetherby and Barry Prizant, this checklist screens communication and symbolic behavior in children between 6 and 24 months. It is available for free download from the developers' research site.
Free Language Sample Analysis Software
Language sample analysis is one of the most informative assessment methods an SLP can use, and two software options make it accessible at little or no cost.
SALT Lite: A streamlined version of the Systematic Analysis of Language Transcripts software. SALT Lite allows you to transcribe and analyze language samples with basic metrics. It is available through the SALT Software website.
CLAN (Computerized Language Analysis): Part of the CHILDES (Child Language Data Exchange System) project hosted at Carnegie Mellon University, CLAN is a free, open-source program for transcribing and coding language data. It is particularly useful for researchers and clinicians analyzing child language development.
Additional Free Informal Resources
Beyond formal screening tools and software, several organizations publish checklists, severity scales, and observation guides that SLPs can download and use immediately.
ASHA Practice Portal Checklists: The American Speech-Language-Hearing Association maintains its Practice Portal with evidence-based resources, including assessment guidance documents and clinical checklists organized by disorder area.
State Early Intervention Screening Forms: Most states publish their own developmental screening forms for Part C referrals. These are typically available as PDFs on state department of health or education websites.
Open-Access Fluency Severity Scales: Tools like the Stuttering Severity Instrument overview documents and the Overall Assessment of the Speaker's Experience of Stuttering (OASES) summary resources are referenced in peer-reviewed literature and can help guide fluency evaluations.
An Important Caveat
While these resources are genuinely useful, it is worth being candid about their limitations. Most free tools function as screenings or informal measures rather than full standardized assessments. They are excellent for identifying concerns, tracking progress, and supplementing a comprehensive evaluation battery, but they generally do not produce the norm-referenced scores required for eligibility determinations in schools or insurance-based settings. Think of free resources as one layer in a well-rounded assessment approach. Pairing them with standardized instruments gives you the clinical depth needed for defensible diagnostic decisions while keeping costs manageable.
If you are building your assessment library from scratch, exploring the resources above is a practical first step. Understanding how graduate programs prepare students to select and administer these tools can help you feel confident before your first clinical placement.
How to Select the Right Assessment Tool for Your Client
Choosing the right assessment tool is one of the most consequential clinical decisions a speech-language pathologist makes. A poorly matched evaluation instrument can produce misleading scores, delay intervention, and frustrate both clinician and client. The good news: a straightforward decision framework keeps you on track every time.
Start With the Referral Question, Not the Test
A practical rule of thumb experienced SLPs rely on is deceptively simple: let the referral question drive your selection, not the other way around. If a pediatrician refers a three-year-old for "not talking yet," the question points toward expressive language and possibly speech sound development. That narrows your disorder area, which in turn narrows the list of appropriate tools. Reaching for a favorite test first and hoping it answers the clinical question is a common pitfall, especially for newer clinicians building their assessment libraries.
Five Factors That Guide Every Selection
Once you have identified the disorder area, weigh these five factors before pulling a test off the shelf:
Client age and developmental level: Many standardized instruments cover specific age bands. Administering a tool outside its intended range compromises validity and can misrepresent a client's abilities.
Referral question and suspected disorder area: Articulation concerns call for different instruments than fluency or swallowing concerns. Match the tool's construct to the clinical question.
Cultural and linguistic background: Check whether the normative sample includes individuals who share your client's demographic profile. If it does not, interpret standard scores with caution and supplement with informal data, language samples, or dynamic assessment to paint a fuller picture.
Setting constraints: School-based SLPs often face strict time limits and eligibility criteria that favor certain batteries. Hospital clinicians may need bedside-friendly tools. Private practitioners might have more flexibility but tighter budgets. Telehealth settings introduce an additional layer: determine whether the publisher offers an approved digital administration format or whether the tool requires in-person manipulation of physical stimuli like objects, blocks, or picture cards.
Psychometric adequacy: Look at sensitivity, specificity, and the representativeness of the norm sample. High sensitivity means the tool correctly identifies individuals who truly have a disorder; high specificity means it correctly rules out those who do not. Both matter for defensible clinical decisions.
The Telehealth Factor
With remote service delivery continuing to grow, tool selection now includes a technology check. Some major publishers have released digital stimulus books and scoring platforms that comply with standardized administration guidelines. Others have not, meaning you would need to administer those assessments in person or risk invalidating the results. Before scheduling a telepractice evaluation, confirm that every tool in your planned battery has a publisher-approved remote option or an acceptable informal alternative. For clinicians interested in building a remote caseload, our guide on SLP telepractice walks through the setup process step by step.
When Scores Do Not Tell the Whole Story
No single test captures a client's full communicative profile. Even the best-normed standardized instrument reflects one snapshot in a controlled context. Pair formal results with observational data, caregiver interviews, and, where appropriate, dynamic assessment to ensure your conclusions are well-rounded and culturally responsive. This multi-method approach is especially important when the normative sample does not adequately represent your client's background.
If you are still building your clinical toolkit, our directory of online speech pathology programs can help you compare graduate programs that emphasize hands-on assessment training, giving you a stronger foundation before you enter the field.
Bilingual and Culturally Responsive Assessment Considerations
Assessing bilingual and multilingual clients is one of the most complex responsibilities an SLP faces. Federal law, specifically IDEA's nondiscriminatory assessment mandate, requires that evaluations be conducted in the child's dominant language or mode of communication and that no single procedure may serve as the sole criterion for eligibility. ASHA's cultural competence guidelines reinforce this standard, calling on clinicians to use assessments that account for linguistic and cultural diversity. Meeting these requirements takes deliberate planning, the right tools, and a clear understanding of what those tools can and cannot tell you.
Bilingual Assessment Tools Available in 2026
Several standardized instruments are designed specifically for Spanish-English bilingual populations:
BESA (Bilingual English-Spanish Assessment): Published by Brookes Publishing, normed on bilingual children ages 4;0 to 6;11, with updated norms as of 2022. BESA is unique because it was developed from the ground up with bilingual norms rather than adapted from a monolingual English test.1
CELF-5 Spanish: Published by Pearson Clinical for ages 5;0 to 21;11, with norms updated in 2019. It is one of the most widely used Spanish-language tools, with a reported usage rate above 91 percent among SLPs who evaluate Spanish-speaking clients.1
ROWPVT-4 Spanish: Published by Super Duper Publications for ages 2;0 to 19;11, normed in 2016, and refreshed on a digital platform in 2024.1
PLS-5 Spanish: Published by Brookes Publishing for children from birth through 7;11, with norms dating to 2011.1
Other tools SLPs may encounter include the Bilingual Verbal Ability Tests (BVAT) and the Systematic Culturally Responsive Evaluations and Assessment Measures in SLP, sometimes referred to as SCREAMS, a framework that guides clinicians through equitable evaluation practices.
Translated Tests vs. Properly Normed Bilingual Tests
This distinction is critical. A test that has simply been translated from English into another language, without being re-normed on speakers of that language, can easily misidentify typical bilingual language patterns as disorders.2 Code-switching, cross-linguistic transfer, and distributed vocabulary (where a child knows some words in one language and different words in the other) are all normal features of bilingual development. Only instruments normed on bilingual populations can account for these patterns. When you rely on a translated-but-not-re-normed tool, you risk over-identifying bilingual children for services they do not need or, conversely, under-identifying children who do.
Best Practices for Equitable Evaluation
Even with the right standardized tools, a single test score is never enough. Recommended best practices include:
Evaluate in both languages whenever possible, collecting samples and scores from each to build a complete profile of the client's communicative abilities.
Use trained interpreters who understand assessment protocols, not family members or untrained staff. The interpreter should know the purpose of each task and how to deliver prompts without inadvertently cueing correct responses.
Apply dynamic assessment methods to distinguish a true language disorder from a language difference. Dynamic assessment measures a client's ability to learn with support, which is far more telling than a static score in one language.
Research from the Texas Speech-Language-Hearing Association highlights how frequently monolingual SLPs rely almost exclusively on English-language instruments when evaluating bilingual students, with English tools used in nearly 97 percent of cases.1 That figure underscores the urgency of integrating bilingual-specific measures and collaborative approaches into routine practice.
The Gap Beyond Spanish
While Spanish-language tools have expanded considerably, standardized assessments for other high-need languages, including Mandarin, Arabic, and Vietnamese, remain extremely limited. Only about 8 percent of SLPs report that the multilingual assessment tools currently available are adequate for their caseloads.1 For clients who speak these languages, clinicians often need to combine interpreter-assisted informal assessment, language sampling, parent and teacher interviews, and dynamic assessment tasks to build a defensible evaluation. Open-access resources such as School-Age Language Assessment Measures (SLAM) can supplement the process by providing structured tasks that do not depend on English-only norms.
Culturally responsive assessment is not an optional add-on. It is a professional and legal obligation. As you build your clinical skill set, whether in graduate school or early in your career, developing comfort with bilingual SLP certification methods will make you a stronger, more ethical clinician and a better advocate for every client on your caseload.
Did You Know?
Research shows that applying English-only norms to bilingual children can inflate overidentification rates by two to three times compared to monolingual peers. To avoid misdiagnosis, SLPs should pair standardized scores with dynamic assessment and language sampling conducted in both languages, which is considered the evidence-based approach for accurate evaluation of bilingual populations.
Telehealth and Digital Assessment Adaptations for 2026
The rapid expansion of telepractice in speech-language pathology has pushed publishers, clinicians, and professional organizations to rethink how assessments are delivered. If you are preparing for a career in SLP, understanding which tools translate well to a virtual environment, and which do not, is now an essential part of your clinical toolkit.
ASHA's Telepractice Standards for Assessment
ASHA's current guidance is clear: telepractice services must be equal in quality to what a client would receive in person.1 That standard applies to evaluation just as much as it applies to treatment. Before conducting a remote assessment, clinicians must confirm that the evaluation is clinically appropriate for the individual client and that the selected tools remain valid when administered through technology.1 ASHA also requires informed consent from the client or caregiver and thorough documentation of any modifications made to standard administration procedures.1 These requirements protect both the client and the clinician by ensuring that telepractice results are defensible and meaningful.
ASHA continues to advocate for expanded telehealth coverage and payment parity, signaling that remote assessment is not a pandemic-era stopgap but a permanent part of the profession's future.2 For students considering this growing service model, our guide on SLP telepractice walks through how to build a remote caseload from the ground up.
Publisher-Approved Remote Administration
Several major test publishers have released official guidance for telepractice administration of their most widely used instruments. Pearson's Q-global platform, for example, supports digital delivery of the CELF-5, allowing clinicians to share stimulus materials on screen while scoring responses in real time. Digital stimulus books for the GFTA-3 similarly enable remote articulation testing without mailing physical materials. Not every subtest within a given instrument is approved for remote use, however. Subtests that rely on physical manipulatives, such as block design tasks or object manipulation, may need to be omitted or replaced with observational data, and clinicians should document those changes.
When using any standardized tool via telehealth, always check the publisher's most current administration manual for remote-specific instructions. Guidelines can change between editions, and relying on outdated permissions can compromise the validity of your results.
Practical Adaptations That Work
Experienced telepractice clinicians have developed a set of reliable strategies for making remote evaluations run smoothly:
Screen-sharing stimulus books: Presenting visual stimuli through screen share keeps the child's attention focused and allows the clinician to control pacing.
On-site facilitator: For younger children, having a parent, teacher, or aide present on the client's end helps manage materials, redirect attention, and position the camera so the clinician can observe oral structures.
Session recording for scoring review: Recording the session (with appropriate consent) lets clinicians replay responses to verify transcription accuracy, a significant advantage over in-person testing where you score in the moment.
Dual-monitor setup: Using two screens, one for the video call and one for the scoring platform, reduces toggling and keeps the interaction feeling natural.
Assessments That Adapt Poorly to Telehealth
Not everything can move online. Oral-mechanism exams require close visual inspection of structures and sometimes tactile cueing, making them difficult to conduct with a standard webcam. Feeding and swallowing assessments, including clinical swallow evaluations and instrumental procedures like FEES or modified barium swallow studies, inherently require the clinician to be physically present. Clinicians working in hospital SLP settings will encounter these limitations most frequently. Play-based evaluations for toddlers and very young children also lose critical observational data when conducted remotely, since the clinician cannot directly manipulate toys or interact within the child's physical space.
For these assessment types, a hybrid model is often the best solution: conduct what you can remotely and schedule targeted in-person sessions for components that demand hands-on interaction.
Emerging Digital-First Tools
A growing number of assessment platforms are being designed from the ground up for digital delivery rather than adapted from paper-based predecessors. iPad-based articulation screeners, for instance, use built-in audio recording and automated phoneme tracking to streamline the screening process. Some newer language sampling apps allow clinicians to elicit, record, and begin transcribing spontaneous speech within a single interface, whether the session happens in person or over video.
These tools are still relatively new, and clinicians should evaluate their psychometric properties carefully before relying on them for eligibility decisions. That said, the trend is unmistakable: the next generation of SLP assessments will increasingly be built for screens, not just adapted to them. Students entering the field now will benefit from gaining comfort with both traditional and digital-first instruments during their graduate training.
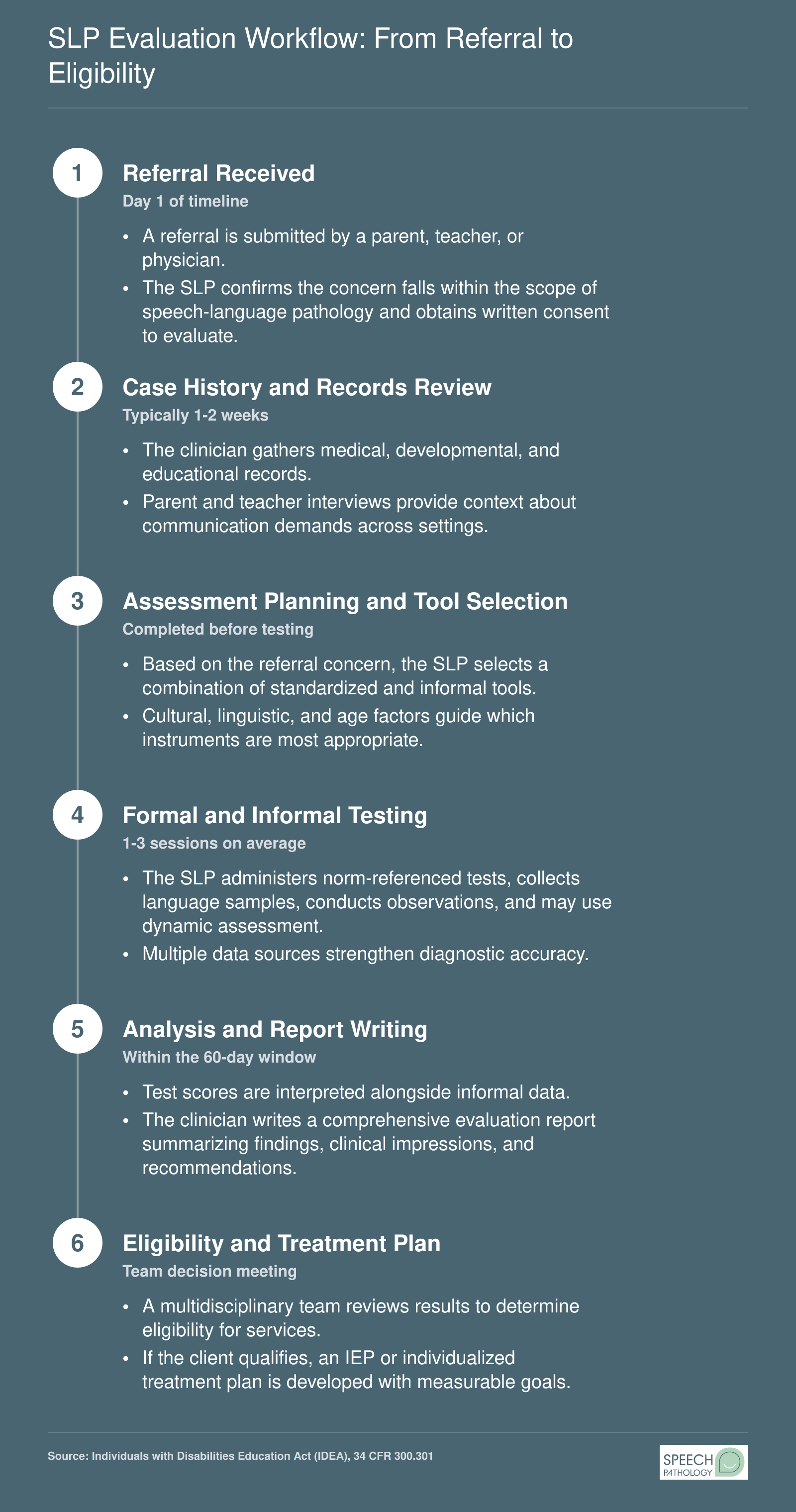
SLP Evaluation Workflow: From Referral to Eligibility
Understanding the full evaluation workflow helps you see exactly where each assessment tool fits into clinical practice. Under IDEA, school-based evaluations must be completed within 60 calendar days of receiving parental consent, though some states set shorter windows. Here is the standard six-step process most SLPs follow when moving a client from initial referral to a finalized treatment plan.
Frequently Asked Questions About SLP Assessment Tools
Whether you are a graduate student preparing for your first clinical placement or a working SLP expanding your evaluation toolkit, the questions below cover the essentials. Each answer connects back to topics explored earlier in this guide, so you can jump to the relevant section for deeper detail.
What assessment tools do speech-language pathologists use most often?
SLPs most frequently use a combination of standardized norm-referenced tests, criterion-referenced measures, and informal tools such as language samples and observation checklists. Common go-to instruments include the Clinical Evaluation of Language Fundamentals (CELF), the Goldman-Fristoe Test of Articulation, and the Peabody Picture Vocabulary Test. The specific mix depends on the client's age, diagnosis, and setting. See the Standardized Assessment Tools by Disorder Area section above for a full breakdown.
What is the difference between formal and informal SLP assessments?
Formal (standardized) assessments are norm-referenced tests administered under strict protocols, producing scores you can compare against age-matched peers. Informal assessments, including language samples, dynamic assessment tasks, and clinical observation, are more flexible and capture real-world communication. Best practice calls for using both types together. The Formal vs. Informal SLP Assessments infographic earlier in this guide offers a side-by-side comparison of when to use each approach.
What are the best free speech and language assessment tools?
Several respected tools are available at no cost. The Communication Function Classification System, open-access language sample analysis programs like SALT and CLAN, and screeners published by university clinics are all widely used. ASHA also shares free practice resources, and many test publishers offer sample protocols. The Free and Low-Cost SLP Assessment Resources section above lists additional options organized by disorder area and population.
Are there SLP assessment tools available in Spanish or other languages?
Yes. Tests such as the Bilingual English-Spanish Assessment (BESA), the Preschool Language Scales (Spanish edition), and the CELF in Spanish are commercially published. However, translated tests are not automatically equivalent to their English versions because cultural and linguistic norms differ. SLPs should also consider dynamic assessment and parent interview protocols when working with multilingual clients. The Bilingual and Culturally Responsive Assessment Considerations section covers this topic in depth.
How do SLPs choose the right evaluation tool for a client?
Tool selection starts with the referral question, the client's age, language background, and the communication domain in question (articulation, language, fluency, voice, or swallowing). SLPs review each test's normative sample to confirm it represents the client's demographic, check psychometric properties like reliability and validity, and factor in practical constraints such as time and cost. The How to Select the Right Assessment Tool section walks through this decision process step by step.
Can standardized SLP assessments be administered via telehealth?
Some standardized tests now have publisher-approved telehealth administration guidelines, and platforms like Q-interactive support remote delivery of select instruments. However, not every test has been validated for virtual use, so SLPs must verify publisher permissions and document any modifications. Informal tools such as language sampling often adapt more easily to video sessions. The Telehealth and Digital Assessment Adaptations section earlier in this guide details current best practices for 2026.
What standardized tests are used for articulation and language disorders in children?
For articulation, the Goldman-Fristoe Test of Articulation (GFTA-3) and the Arizona Articulation and Phonology Scale are among the most widely administered. For language, the CELF-5, the Preschool Language Scales (PLS-5), and the Test of Language Development (TOLD) are commonly selected. Many clinicians pair these with informal measures such as connected speech samples to build a complete clinical picture. The Standardized Assessment Tools by Disorder Area section provides a broader directory.