Accurate assessment is the foundation of ethical bilingual practice, yet it remains one of the most challenging tasks an SLP faces. Choosing the right tools, understanding their norming populations, and pairing formal measures with dynamic assessment strategies all play a role in distinguishing a true communication disorder from the expected patterns of bilingual language development. For students building toward a career as a bilingual speech pathologist, mastering these assessment strategies early is essential.
The Difference-vs-Disorder Framework
When a bilingual child is referred for evaluation, the first clinical question is whether the observed language patterns reflect a language difference or a genuine disorder. A language difference describes the predictable features of someone acquiring two (or more) languages simultaneously or sequentially: code-switching, transfer patterns between languages, and uneven vocabulary distribution across languages are all typical. A true disorder, by contrast, affects both languages and persists regardless of the amount of input or instruction a child receives.
SLPs use the difference-vs-disorder framework to avoid over-identifying bilingual children for services they do not need, or under-identifying children who do. Tools designed for bilingual populations, combined with language sampling in both languages and caregiver interviews, give clinicians the evidence they need to make that distinction confidently.
Key Bilingual Assessment Instruments
Several standardized tools have been developed or adapted specifically for bilingual Spanish-English populations. Each targets different age ranges and language domains.
- Bilingual English-Spanish Assessment (BESA): Designed for children ages 4 through 6;11, the BESA evaluates morphosyntax, semantics, and phonology in both English and Spanish. It was normed on bilingual children, which makes its scores more clinically meaningful for this population than translated English-only tests.
- CELF-5 Spanish: Covers ages 5 through 21 and measures core language skills including sentence comprehension, word structure, and formulated sentences. It was normed on monolingual Spanish speakers, so clinicians should interpret scores cautiously for simultaneous bilinguals.
- PLS-5 Spanish: Appropriate for birth through age 7;11, this tool assesses auditory comprehension and expressive communication. It is commonly used in early intervention settings.
- TOLD-P:5 Spanish: Targets ages 4 through 8;11 and evaluates semantics, morphology, and syntax. Like the CELF-5 Spanish, its norms are based on monolingual Spanish-speaking children.
When selecting any of these instruments, SLPs should review the norming sample carefully and consider whether the child's language profile matches the population on which the test was standardized. For a broader look at formal and informal measures, explore our SLP Assessment Tools & Evaluation Resources guide.
Translated Parent Questionnaires and Intake Forms
Parent report is an essential complement to direct testing, especially for toddlers and preschoolers whose performance can vary dramatically across settings. Several widely used questionnaires are available in Spanish and other languages.
- ASQ (Ages and Stages Questionnaires) in Spanish: A developmental screening tool covering communication, gross motor, fine motor, problem-solving, and personal-social domains. Many early intervention programs use the Spanish version as a first-line screener.
- MacArthur-Bates Communicative Development Inventories (CDI) adaptations: The CDI has been adapted into more than 100 languages and dialects worldwide. Spanish adaptations (Inventarios del Desarrollo de Habilidades Comunicativas) allow caregivers to report vocabulary and gesture use in their home language, giving SLPs a clearer picture of total conceptual vocabulary.
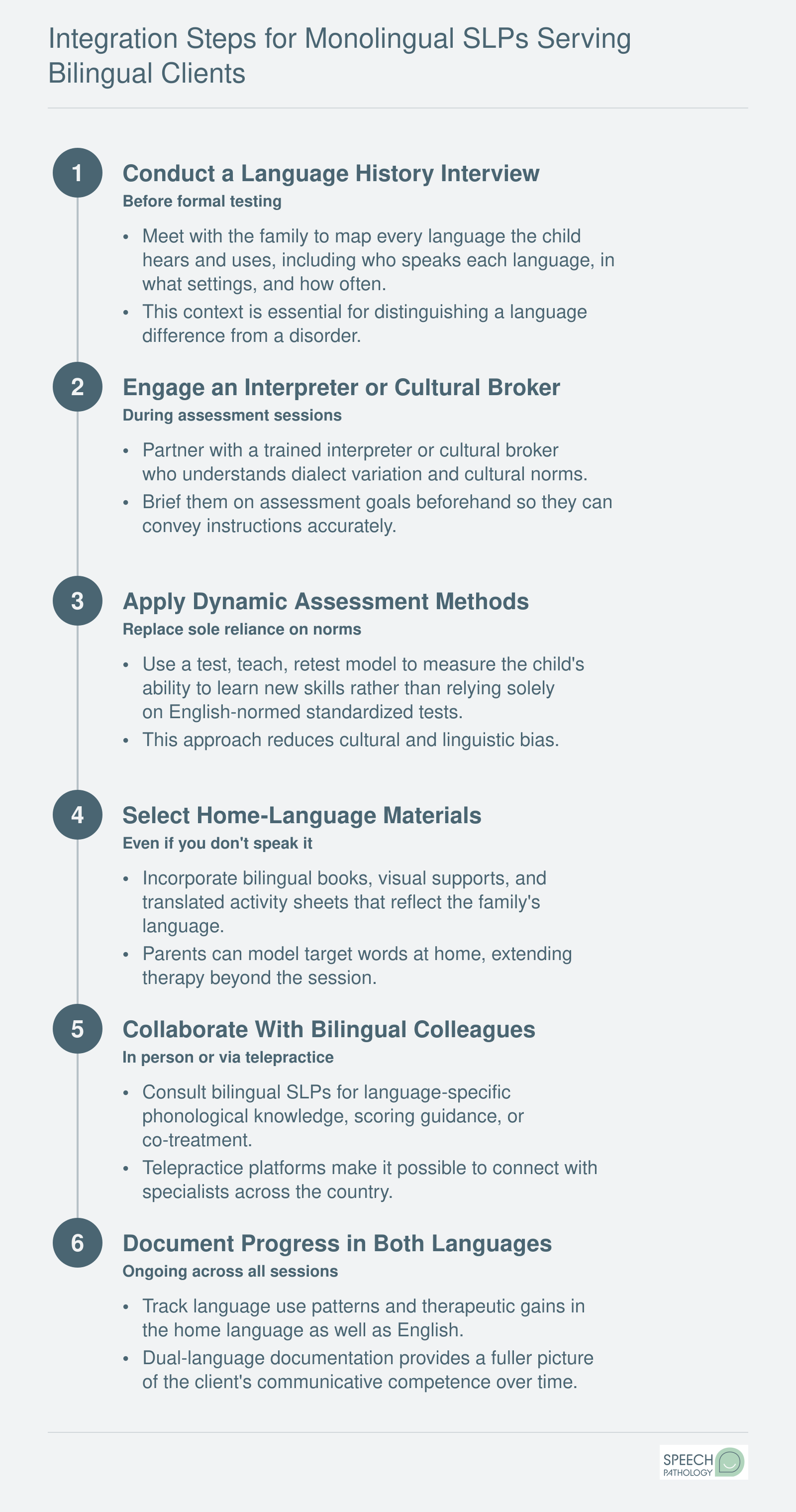
- Freely available parent interview protocols: Organizations such as ASHA and several university clinics offer downloadable bilingual case history forms and language-use questionnaires that help clinicians map a family's language environment, including who speaks which language, how often, and in what contexts.
These questionnaires work best when administered in the language the caregiver is most comfortable using, ideally by a bilingual clinician or trained interpreter.
Why Direct Translation of English-Normed Tests Falls Short
One of the most common missteps in bilingual assessment is simply translating an English-normed test into another language and using the original scoring tables. ASHA's position statements are clear on this point: translated tests do not account for the phonological, morphological, or cultural differences between languages, and their norms do not apply to a population they were never designed to measure. A translated test can over-identify typical bilingual patterns as deficits or miss genuine areas of concern.
ASHA recommends dynamic assessment as a powerful alternative or supplement. In dynamic assessment, the clinician teaches a skill during the evaluation session and then measures how quickly and effectively the child learns it. Because this approach evaluates a child's ability to learn rather than what they already know, it reduces cultural and linguistic bias and provides clinically rich information about a child's true language-learning potential.
Combining standardized bilingual instruments, caregiver questionnaires, language samples in both languages, and dynamic assessment tasks gives SLPs the most complete and equitable picture of a bilingual child's abilities. For students exploring this career path, building competence in these assessment strategies early, whether through coursework, clinical practica, or continuing education, positions you to serve diverse populations with confidence from day one.