What SLPs and Future Clinicians Need to Know About Reimbursement Challenges, Provider Exits, and Child Access to Care
By Benjamin Thompson, M.S., CCC‑SLPReviewed by SLP Editoral TeamUpdated June 14, 202623 min read
Points of interest…
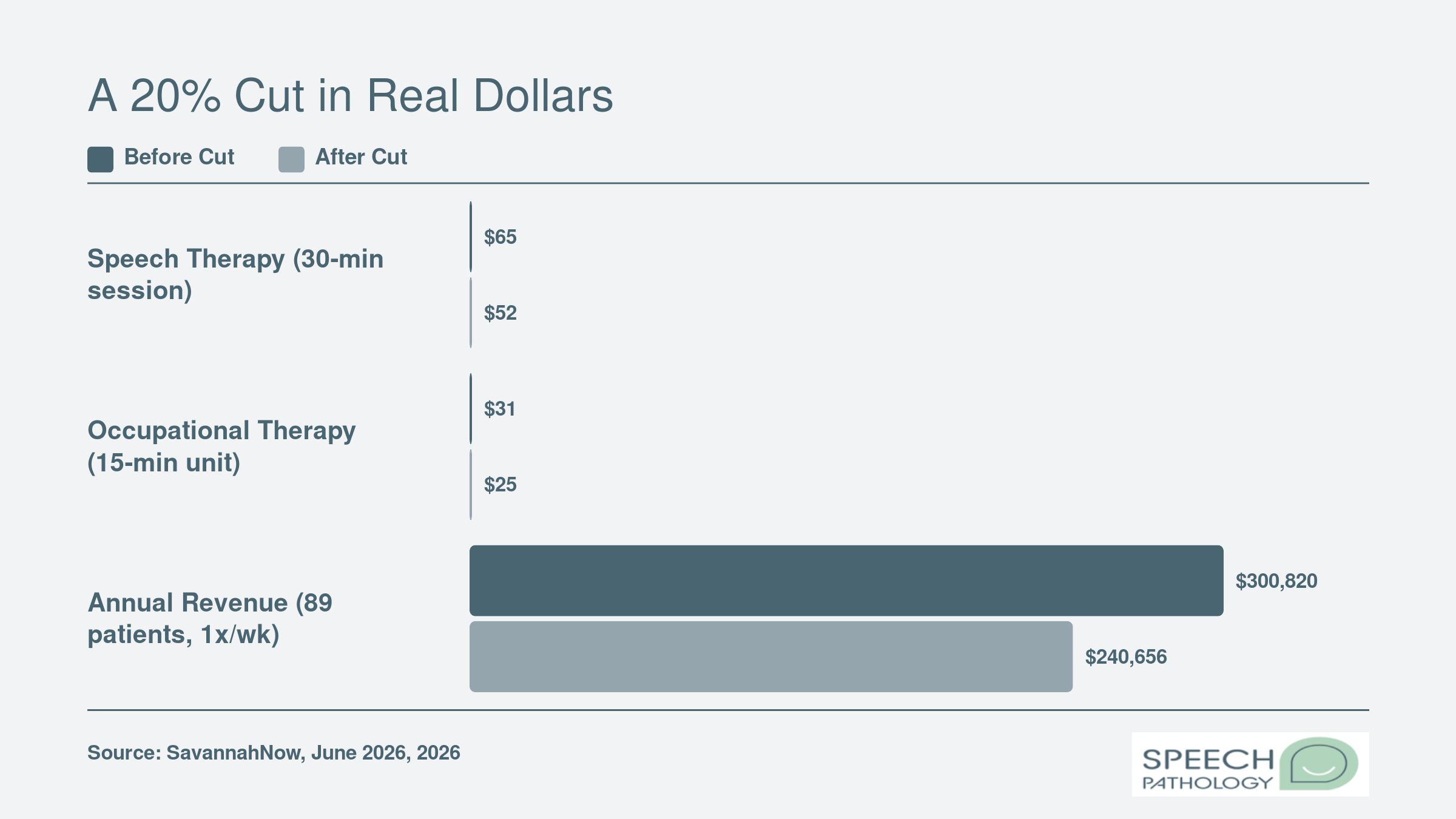
CareSource reduced Georgia pediatric therapy reimbursement by 20%, cutting a 30-minute speech session from $65 to $52.
Chatterbox Pediatric Therapy will stop accepting CareSource patients in August 2026, affecting 89 children.
The One Big Beautiful Bill Act proposed nearly $1 trillion in Medicaid cuts, prompting ASHA advocacy.
Millions of U.S. children rely on Medicaid for speech therapy each year. When reimbursement rates drop, as they did this spring for Georgia providers contracted with CareSource, those services can abruptly disappear. Chatterbox Pediatric Therapy saw its 30-minute speech session payment fall from $65 to $52, a 20% cut that pushed the clinic to plan an exit from the CareSource network by August 2026.1
The Georgia case follows a national pattern: as managed care organizations trim therapy rates, small pediatric practices face a choice between absorbing losses and stopping care for Medicaid patients. Clinics that do walk away leave families scrambling for alternatives, often in areas with few options. For SLPs considering careers in states like Georgia, understanding speech pathology programs in Georgia and local reimbursement landscapes is increasingly essential.
Rate cuts are not abstract policy debates. They reshape where SLPs can work, how graduate students find clinical placements, and whether children receive consistent care. The economic pressure has become a core clinical reality.
What's Happening With Medicaid Reimbursement for Speech Therapy?
Between 2024 and 2026, Medicaid managed care organizations reduced reimbursement for therapy services by 5% to 20%, leaving many pediatric speech-language pathologists scrambling to cover rising practice costs.1 For a profession built on consistent, long-term relationships with children, these cuts don't just shrink paychecks. They disrupt care.
The Medicaid-MCO Connection: A Two-Tier System
Medicaid reimbursement for pediatric speech therapy isn't set by a single national rate. Each state establishes its own fee schedule, and the federal government matches a percentage of those costs. However, most states now contract with managed care organizations (MCOs) to administer benefits for many enrollees. These private insurers, like CareSource in Georgia, can pay providers at rates different from the state fee schedule. Federal regulations (42 C.F.R. Part 438) don't require MCOs to match fee-for-service rates.1 Unless a state creates a rate floor, MCOs have broad latitude to negotiate lower reimbursement.
That creates a two-tier reality. When a state like North Carolina mandates that MCOs pay at least 100% of the fee-for-service rate for behavioral health services, including therapy, providers get predictable income.2 But in many states, no such floor exists, and rates vary wildly. New York's managed care plans, for example, pay considerably lower than fee-for-service, according to state reports, and the rates are set through contract negotiations rather than tied to any benchmark.3 For solo or small speech therapy vs occupational therapy practices with limited bargaining power, that often means accepting whatever the MCO offers or walking away.
A National Pattern of Declining Reimbursement
The recent cuts aren't isolated. Across the country from 2024 to 2026, MCO reimbursement for therapy providers has declined by 5% to 20%, even as costs for rent, supplies, and staff salaries climb.1 This structural squeeze reflects a broader push by states and insurers to control Medicaid spending. Yet for speech-language pathologists, whose services are already reimbursed at rates far below comparable medical specialties (a gap visible in speech language pathologist salary data), each percentage point cut forces tough choices: reduce hours, drop Medicaid patients, or close entirely.
Why MCO Cuts Hit Speech Therapy Especially Hard
Speech therapy relies on frequency and relationship-building. A child with an articulation disorder or autism often needs weekly sessions over months or years. When a clinic can no longer afford to accept Medicaid-funded patients, those children lose access to a trusted provider mid-treatment. MCOs cite national trends and responsible use of taxpayer dollars, but providers argue that short-term savings risk long-term harm, both to patients and to the therapy workforce. Without rate floors, MCOs can unilaterally impose reductions with little notice, as clinics in Georgia experienced when CareSource moved to 80% of the state schedule.
The Rationale vs. the Reality
CareSource's justification, reflecting national trends and ensuring fiscal responsibility, echoes language used by MCOs nationwide. But for pediatric speech therapy, where progress is built on consistency, the real cost of a 20% cut isn't captured in a budget line. It's measured in delayed milestones, lost clinical placements for future SLPs, and clinics that stop accepting the very children who need them most.
Georgia Case Study: How One Managed Care Cut Is Forcing Clinics Out
When a major insurer slashes reimbursement by 20%, pediatric therapy clinics face a wrenching tradeoff: accept a rate that may not cover costs, or stop serving children who depend on their care. In Georgia, that decision is now playing out in real time, as a managed care company's rate cut forces providers to choose between financial survival and patient access.
A Sudden Shift in Reimbursement
In spring 2026, CareSource, a large Medicaid managed care plan in Georgia, notified many therapy providers that their rates would drop from 100% to 80% of the state's Medicaid fee schedule.1 The change was framed as a reflection of "national trends" and a way to "help ensure taxpayer dollars are used responsibly as costs intensify," according to the company. For speech-language pathologists (SLPs), the math was stark: a standard 30-minute speech therapy session that previously reimbursed around $65 under Georgia Medicaid would now bring in roughly $52. Occupational therapy units, billed at about $31 per 15-minute segment, would fall to around $25.
Chatterbox Pediatric Therapy: Choosing to Walk Away
For Beth Brinkley Rollins, owner of Chatterbox Pediatric Therapy in Pooler, the cut threatened the clinic's viability. Out of 350 to 400 total patients, 89 were CareSource beneficiaries, many of them children with autism who need consistent, long-term speech therapy for autism.1 Rollins determined that absorbing the lower rates would undermine her ability to pay staff and maintain quality. Instead of accepting the reduced payments, she plans to stop taking CareSource patients altogether starting in August 2026. "Building relationships with pediatric patients is critical to progress," Rollins has noted, and forcing families to find new providers disrupts that hard-won continuity. Cases like this highlight the financial pressures facing any SLP private practice owner navigating Medicaid contracts.
Joyce Psychology & Wellness: A Contract Terminated
In Savannah, Joyce Psychology & Wellness, a larger practice with 19 providers and nearly 7,000 patients over three years, faced a similar ultimatum. The clinic received notice of the 20% cut in March, with an effective date of May 11, 2026. After formally rejecting the new terms, the clinic's contract with CareSource was terminated.1 Leaders there argue that such cuts don't just squeeze individual businesses; they threaten the entire pediatric therapy network. When clinics close or drop Medicaid, the shortage affects all children in the region, regardless of their own insurance, because the remaining providers become overwhelmed.
The Ripple Effects on All Children
Both clinics underscore a point that reaches far beyond Georgia: pediatric therapy relies on trust and familiarity. For children with autism, who may take months to feel safe with a therapist, switching providers can stall or reverse progress. When reimbursement rates become unsustainable, it is the most vulnerable patients who lose access first. The Georgia dispute illustrates how a single policy change can cascade into clinic closures, fractured care, and deeper inequities for families who already navigate complex systems.1
A 20% Cut in Real Dollars
The CareSource reduction in Georgia cut Medicaid reimbursement for therapy providers from 100% to 80% of the state fee schedule. For a clinic like Chatterbox Pediatric Therapy, the per-session drop adds up to an estimated annual revenue shortfall of $60,164 for its 89 CareSource patients, assuming once-weekly sessions.
Which States Are Cutting or Raising SLP Medicaid Rates?
Staying informed about Medicaid reimbursement rates means choosing between two distinct approaches: diving directly into state fee schedules yourself or relying on curated updates from professional associations. Both paths have value, but knowing when to use each can save time and prevent costly surprises for your practice or clinical placement planning.
Tracking State-Level Changes
For the most accurate and immediate data, nothing beats going straight to the source. Each state's Medicaid agency publishes fee schedules that detail exactly what speech-language pathology services are reimbursable and at what rate. Start by searching for "[your state] Medicaid speech therapy fee schedule." Most state health or human services departments post these online in searchable PDFs or Excel files. Bookmark the page and check quarterly, since states often update rates at the start of a fiscal year or calendar year.
Our scan of several states for 2024 through 2026 reveals a common theme: rate stability. Florida, Pennsylvania, Mississippi, Kentucky, and South Dakota all show no documented cuts or increases to their Medicaid fee schedules for speech-language pathology during this period.12345 This doesn't mean every provider in those states is unaffected. Managed care organizations (MCOs) may administer their own networks and reimbursement rates, as seen in the recent Georgia case. But the state-level floor has held firm in many places.
At the federal level, the 2026 Medicare Fee Schedule for speech-language pathologists brought a modest increase of roughly 2.5% to 3.8%.6 While Medicare is distinct from Medicaid, this federal benchmark can influence state decisions and MCO negotiations. Still, it's not a guarantee that Medicaid rates will follow, and in fact most state Medicaid programs haven't mirrored that upward adjustment.
Using Professional Association Resources
If manually checking dozens of state websites feels daunting, lean on the advocacy work of organizations like the American Speech-Language-Hearing Association (ASHA). ASHA regularly publishes state-by-state reimbursement comparisons, policy alerts about proposed cuts or increases, and summaries of legislative actions that affect SLP services. Their website (asha.org) is a first stop when you need a big-picture view without getting lost in bureaucratic language.
ASHA's updates often highlight patterns you might miss on your own, for example, clusters of states that freeze rates during economic downturns, or a trend of MCO-level reductions even when state fee schedules appear stable. These summaries also connect rate changes to broader workforce impacts, such as clinic closures or provider shortages, which can directly affect your job market and clinical training opportunities. For students still planning their path, understanding how communication disorders degree careers intersect with reimbursement policy is increasingly important.
Searching Legislative and Administrative Actions
Rate adjustments aren't always labeled neatly as "Medicaid reimbursement." Many take the form of line items in state budget bills, administrative code revisions, or early intervention program reauthorizations. To catch these, go to your state legislature's website and search for terms like "Medicaid speech therapy rate increase," "Early Intervention reimbursement," or "pediatric therapy services." Bill tracking systems let you see what passed and what stalled, giving you early warning of pending changes.
This direct legislative monitoring is especially critical if you work in or plan to work in states where managed care penetration is high, because MCO rate cuts, like those in the Georgia CareSource example, often happen with less public notice than state-level fee schedule updates. SLPs who understand the SLP scope of practice are better positioned to articulate why adequate reimbursement matters and to advocate effectively at the policy level.
Ask Yourself
How Rate Cuts Affect Children and Families
What actually happens to a child's speech therapy when a clinic decides it can no longer afford to accept Medicaid? The answer is rarely a simple transfer to a new provider. Instead, families face a cascade of disruptions that can stall hard-won progress and erode their child's confidence just when consistency matters most.
Losing a trusted therapist
For children, speech therapy is not just a clinical appointment. It is a relationship built over months or years. When a clinic drops Medicaid, the therapist a child knows and trusts may suddenly become inaccessible. Beth Brinkley Rollins, owner of Chatterbox Pediatric Therapy in Georgia, recently announced that her clinic will stop accepting CareSource patients starting in August 2026 rather than accept a 20% reimbursement cut.1 That one decision displaces 89 children from a provider who knows their goals, triggers, and progress patterns. Rebuilding that therapeutic bond with a new clinician often sets children back, sometimes undoing gains in articulation, social communication, or feeding skills. This disruption is especially acute for children on the autism spectrum, who depend on predictable routines and familiar faces to make autism speech therapy techniques effective.
Emerging waitlists and reduced availability
Fewer Medicaid-accepting slots don't just inconvenience families; they create real access gaps. In Texas, where therapy rates are widely seen as inadequate, many SLPs warn they may be forced to opt out of the program altogether if reimbursement falls further.2 Even when clinics stay in network, they often cap the number of Medicaid patients they can serve, and the wait for an opening can stretch into months. While state-level waitlist data is notoriously hard to compile, professional networks and school district special education directors are already documenting a troubling rise in families who cannot find timely care.
Connecticut's 2026 Medicaid Rate Evaluation Process acknowledges this tension, setting criteria that include "support member access" alongside cost containment, but the outcome of those reviews is still uncertain.3 North Carolina recently removed the ASHA CCC requirement for Medicaid provider enrollment, a move intended to ease administrative burdens and expand the provider pool.4 Yet if rates remain flat or decline, more SLPs may still choose to leave the network.
The ripple effect on all families
Rate cuts don't only affect families on Medicaid. When a pediatric therapy practice relies heavily on Medicaid revenue, a 20% drop can jeopardize the entire clinic's finances. Clinic owners often respond by reducing hours, laying off staff, or shutting their doors entirely, decisions that shrink the overall supply of pediatric SLPs in a community. In Georgia, providers argued that clinic closures would hurt children "regardless of insurance," because even families with private pay must compete for a diminished pool of available slots.1 Understanding these financial pressures is one reason aspiring SLPs benefit from studying public health speech-language pathologist career paths, where systemic advocacy and policy literacy are core skills.
Early intervention at risk
Medicaid is the primary payer for early intervention services for children under three, a developmental window when speech therapy can prevent long-term academic and social difficulties. When reimbursement cuts force providers out of the system, families may wait longer for evaluations and treatment, missing the period when the brain is most responsive to language intervention. National Medicaid enrollment dipped by 7.6% in fiscal 2025, but a forecasted flat trend for 2026 suggests demand for pediatric speech services won't drop enough to absorb the loss of providers.5
Disruption of care: Abrupt therapist changes can reverse months of speech progress.
Long waitlists: Even if a new provider exists, families may wait weeks or months for an appointment.
Financial squeeze: Parents who turn to private pay or travel farther often face higher out-of-pocket costs.
Missed milestones: Delayed early intervention can mean children enter school behind their peers in language and social skills.
Impact on SLP Private Practices, Schools, and Hospitals
When Medicaid reimbursement shrinks, the pain isn't distributed equally across speech-language pathology settings. Understanding where the biggest vulnerabilities lie helps clinicians, students, and advocates target their efforts and anticipate career impacts.
Private Practices: The Hardest Hit
Private practices that rely heavily on Medicaid face an immediate existential threat. A 20% rate cut can turn a sustainable business into a losing one, especially when overhead costs continue to rise. These clinics often cannot simply "absorb" the loss; they must either stop accepting new Medicaid patients, shift to a private-pay model, or close entirely. That means families with low incomes lose access to the consistent, specialized speech therapy their children need. Anyone considering how to start an SLP private practice should recognize that private practices lack the subsidies and diversified revenue streams protecting larger institutions, making them uniquely fragile in the current reimbursement climate.
School-Based Medicaid Billing: Hidden Funding at Risk
Schools do bill Medicaid for speech-language pathology services provided to eligible students, though many SLPs are unaware of this backend funding mechanism. Under the School-Based Medicaid program, districts can claim reimbursement for medically necessary therapy delivered during the school day. These dollars flow into the district budget and often help cover SLP salaries and program costs. When reimbursement rates drop, districts lose a critical revenue source, which can lead to hiring freezes, larger caseloads, or fewer therapy sessions. Because special education mandates require services, schools cannot simply eliminate speech therapy, but cuts can degrade the quality and frequency of interventions.
Hospital outpatient units that offer pediatric speech therapy operate in a complex cost environment. While they may serve some Medicaid patients, they often cross-subsidize low-margin services with higher-reimbursing procedures. When Medicaid rates fall further, speech therapy can become a financial drain. Hospitals may respond by reducing clinic hours, limiting the number of Medicaid slots, or moving resources to more profitable services. This doesn't always mean eliminating speech therapy, but it can mean longer wait times and fewer providers, especially for children who need long-term, relationship-based care. Each of these dynamics plays differently depending on the SLP career settings a clinician chooses.
The Vulnerability Gap
The contrast is stark: private practices are the most exposed because they depend on a single payer or a narrow mix of payers and lack the financial buffers of hospitals or the legal funding mandates of schools. While school districts and hospitals may weather cuts by tightening budgets elsewhere, private practice owners often face an all-or-nothing choice. This differential explains why rate cuts can quickly wipe out access in some communities while leaving institutional settings relatively, but not completely, unaffected.
What Medicaid Reimbursement Means for SLP Earnings
The Reimbursement-to-Salary Gap
National SLP salary figures can be misleading for pediatric clinicians, whose earnings often fall well below the median when their caseload relies heavily on Medicaid. As reimbursement cuts continue, this gap may grow, making it harder to attract and retain therapists in the settings where children need them most.
How SLPs Can Advocate for Fair Reimbursement
The One Big Beautiful Bill Act proposed nearly $1 trillion in Medicaid funding cuts, prompting the American Speech-Language-Hearing Association (ASHA) to launch a sustained, multi-pronged advocacy response.1 For speech-language pathologists who rely on Medicaid reimbursement, these policy developments are not distant headlines. They directly shape clinic viability, service capacity, and patient access. Knowing how to engage effectively can shift the trajectory of rate decisions in your state.
ASHA's Advocacy Playbook: Tools, Alerts, and Direct Support
ASHA maintains a centralized Medicaid Cuts and Coverage Changes page that tracks federal and state-level threats, offering talking points, legislative templates, and action alerts.1 The ASHA Advocate alert system notifies members when a critical bill or regulatory change requires immediate outreach. SLPs can also connect with the State Advocates for Reimbursement (STARs) program, a network of volunteers who coordinate state-level reimbursement strategy and receive policy briefings. For personalized guidance, ASHA's reimbursement team is reachable at [email protected]. On-demand webinars, such as "Medicaid Advocacy in 2026: Partnerships and Progress" and "Proposed Medicaid Funding Changes Ahead," provide deeper training on navigating complex funding landscapes.
Concrete Steps to Influence State and Federal Policy
Momentum often starts at the state level. SLPs can attend public hearings when Medicaid managed care organizations (MCOs) propose contract renewals and submit written comments during open public-comment periods. Contacting state legislators directly, using ASHA's prepared templates to explain how a proposed cut would reduce service hours or force clinic closures, has proven effective. In Washington, sustained clinician and family advocacy led to a March 2026 reversal of cuts to school-based Medicaid and outpatient adult SLP services.1 North Carolina achieved a similar reversal in December 2025 after provider pushback.2 Joining a state speech-language-hearing association amplifies your reach, as these groups often coordinate sign-on letters, lobby days, and joint media statements. On the federal side, ASHA urges members to respond to action alerts asking legislators to repeal harmful funding provisions.
Using Data to Make the Case: Patient Outcomes and Cost-Effectiveness
Lawmakers are more likely to protect reimbursement when providers can show that services save money downstream. SLPs who systematically document progress metrics, such as reduced communication-related emergency department visits, improved school readiness, or decreased need for special education placements, can turn anecdote into evidence. ASHA encourages members to submit outcome data to state Medicaid agencies as part of formal rate-review processes. Demonstrating that early intervention speech therapy averts costlier long-term care, behavioral interventions, or institutionalization frames reimbursement as an investment rather than an expense. Understanding how SLPs help children on the spectrum through autism speech therapy techniques is one example of the specialized value that outcome data can capture.
Amplifying the Message Through Coalitions
Reimbursement battles are rarely won by one profession alone. Collaborating with occupational therapists, physical therapists, psychologists, and parent advocacy organizations creates a unified voice that legislators find harder to ignore. Joint letters, shared testimony, and coordinated media outreach can highlight the ripple effects of rate cuts across the entire pediatric therapy ecosystem. Parent-led groups, in particular, bring powerful personal stories that humanize the dollars-and-cents debate. ASHA's resources often include guidance on forming and participating in such coalitions, recognizing that sustained partnerships multiply advocacy impact.
What This Means for SLP Students and Future Clinicians
Clinical Placements Are on the Line
When clinics stop accepting Medicaid or close outright, the ripple effects hit SLP graduate students hard. Pediatric SLP externships become scarce. A clinic like Chatterbox Pediatric Therapy, which plans to drop CareSource patients this year, may scale back overall caseloads or shut down entirely. That means fewer opportunities for students to gain hands-on experience with the early intervention and autism populations that form the backbone of pediatric speech pathology training. If you are mapping out your clinical rotations, talk to your program's placement coordinator now about how Medicaid reimbursement trends are affecting site availability in your area.
Insurance Literacy Is a Career Skill
Before you ever sign a job offer, you need to understand the difference between fee-for-service Medicaid and managed care organizations (MCOs). In Georgia, CareSource is an MCO that cut reimbursement to 80 percent of the state Medicaid fee schedule, a move that squeezed clinic margins instantly. Knowing how to read a contract, calculate your break-even rate per session, and compare payer mixes isn't just for private practice owners. It protects your SLP salary and job stability whether you work in a clinic, school, or hospital. Courses in professional issues often touch on billing codes, but students should actively seek out webinars, ASHA resources, and mentorship from working SLPs to build this financial fluency now.
The Job Market Paradox
At first glance, provider exits create short-term demand: if clinics close, the remaining ones may scramble to hire. But that demand is fragile. When reimbursement rates are too low to cover operating costs, even positions that start out promising can evaporate if the business model becomes unsustainable. You may find a job in an underserved rural or urban area, only to see the clinic lose its Medicaid contract a year later. As you evaluate job offers, ask potential employers how reliant they are on Medicaid managed care and whether they have diversified their payer sources. A setting that looks stable on paper might be one rate cut away from layoffs. Comparing speech pathology work environments can help you weigh stability alongside mission. This doesn't mean avoiding Medicaid-based settings altogether. Many are mission-driven and deeply rewarding. But it does mean going in with eyes open.
Advocacy Starts Now
You are entering a profession at a time when reimbursement policy will define the scope of services you can provide. Rather than inheriting a broken system, you can help reshape it. Join ASHA's advocacy network, follow your state association's legislative alerts, and pair your clinical training with an understanding of health policy. When Georgia providers pushed back against the 20 percent cut and some lost their contracts, it illustrated how quickly third-party payer decisions can override clinical judgment. By building advocacy skills early, writing op-eds, attending statehouse days, and documenting patient outcomes to justify funding, you become part of a generation of SLPs equipped to argue for fair rates not as a political extra, but as a professional obligation.
Frequently Asked Questions About Medicaid Rate Cuts and Speech Therapy
The Georgia experience shows what's at stake: when Medicaid reimbursement drops 20%, clinics like Chatterbox Pediatric Therapy can no longer afford to serve the children who depend on them. That loss of access is not theoretical. It disrupts care for dozens of families immediately, with ripple effects across the community.
Whether you are a practicing SLP, a student preparing for your speech pathology internship, or a family navigating the system, staying informed and advocating at the state level is essential. Fair reimbursement is not just about keeping practices open; it is about ensuring every child who needs speech therapy can get it, without gaps or compromises.