How Speech-Language Pathologists Support Children With Autism
A comprehensive guide to evidence-based techniques, therapy settings, costs, and how to track your child's progress
By Benjamin Thompson, M.S., CCC‑SLPReviewed by SLP Editoral TeamUpdated July 17, 202625+ min read
Points of interest…
SLPs treat social communication and pragmatic language in autism, not just articulation or speech clarity.
About 1 in 36 U.S. children is identified with autism spectrum disorder, making early intervention critical for outcomes.
AAC tools do not delay spoken language and give minimally verbal children a reliable way to communicate.
Families can legally combine school based speech therapy with private services to address broader communication goals.
With roughly 1 in 36 U.S. children now identified with autism spectrum disorder, demand for speech-language pathologists trained in social communication intervention has never been higher. Federal data show that speech-language services are among the most common supports provided to autistic students under IDEA, yet many families still assume an SLP's role begins and ends with articulation drills.
The reality is far broader. For children on the spectrum, SLPs target pragmatic language, joint attention, conversational reciprocity, and augmentative communication, often collaborating closely with occupational therapists and speech pathologists as well as behavior analysts. Despite this central role, access remains uneven: session costs, insurance variability, and long waitlists in many regions mean families frequently piece together school-based and private services simultaneously just to maintain adequate frequency.
Why Do Autistic Children Struggle With Speech and Communication?
Understanding why communication is so challenging for children on the autism spectrum is the first step toward providing effective support. The reasons are layered and vary enormously from one child to the next, but they generally fall into a few interconnected categories that speech-language pathologists are trained to evaluate and address.
Speech Delays vs. Social-Communication Differences
One of the most common misconceptions is that autism always means a child cannot talk. In reality, many autistic children develop spoken language on or near a typical timeline, yet they still face significant communication barriers. The distinction lies in pragmatic language, the social "rules" that govern how we use words in context.
A child may have a large vocabulary but struggle with skills like:
Turn-taking: Knowing when to speak and when to listen during a conversation
Reading tone and intent: Interpreting sarcasm, humor, or indirect requests
Making inferences: Understanding what a speaker implies rather than states outright
Adjusting register: Changing how they speak depending on the listener (a peer vs. a teacher, for example)
These pragmatic gaps can be just as isolating as a speech delay. Children with strong vocabularies who miss social nuance are often misunderstood by teachers and peers, and their communication needs may go unrecognized for years.
Sensory and Motor Factors That Compound Communication Barriers
Communication does not happen in a vacuum. For many autistic children, sensory-processing differences and motor-planning challenges create additional obstacles that sit underneath the language difficulty.
Auditory hypersensitivity can make noisy classrooms overwhelming, causing a child to withdraw or shut down rather than engage in verbal interaction. When processing everyday sounds requires extra effort, following spoken language in real time becomes exhausting.
Motor-planning difficulties add another layer. Childhood apraxia of speech, a condition in which the brain struggles to coordinate the precise movements needed for clear speech, co-occurs with autism at higher rates than in the general population. A child with co-occurring apraxia may know exactly what they want to say but be unable to produce the sounds reliably. Apraxia is one of several common speech disorders that an SLP evaluating an autistic child must screen for, looking beyond language comprehension to assess the motor system as well.
The Minimally Verbal Population
Research consistently indicates that roughly 25 to 30 percent of autistic children remain minimally verbal past age five, producing few or no spoken words for functional communication. "Minimally verbal" does not mean a child has nothing to say. It means that spoken language alone is not a reliable channel for them.
This reality underscores why augmentative and alternative communication (AAC) strategies are a core part of the SLP toolkit. For children in this group, the goal is not exclusively to develop spoken words but to build a robust communication system, whatever form that takes. We will look at specific AAC options in a later section.
Communication Challenges Exist Across the Spectrum
It is worth emphasizing that no level of verbal ability makes a child "done" with communication support. A highly verbal teenager who dominates conversations about a favorite topic but cannot navigate a job interview still has a communication need. A preschooler who echoes full sentences from a cartoon but cannot request a snack also has a communication need. The spectrum of challenges is as wide as the spectrum itself, and recognizing that range is essential for anyone considering a career in speech-language pathology.
What Does an SLP Do for a Child With Autism?
One of the most common misconceptions about speech-language pathologists is that they only help children pronounce words more clearly. For children on the autism spectrum, articulation is rarely the primary concern. Instead, SLPs focus on social communication, pragmatic language, and functional communication, helping children learn not just how to speak but how to connect, request, share ideas, and navigate everyday interactions.
SLP involvement with autistic children generally spans four core functions: comprehensive assessment, individualized goal-setting, direct therapy delivery, and interdisciplinary collaboration.1
Comprehensive Assessment
An initial evaluation typically combines standardized testing with naturalistic observation. The SLP may use speech language pathology assessment tools such as the Clinical Evaluation of Language Fundamentals (CELF), the Preschool Language Scales (PLS), or communication-domain scores from the ADOS-2, alongside play-based observation and parent or caregiver interviews. There is no single mandated list of assessment instruments; clinicians select measures based on each child's age, language level, and cultural and linguistic background.1 Current guidelines call for a family-centered, culturally responsive approach, which may include working with interpreters or cultural brokers when needed.
Parents should expect to receive a written report that outlines the child's receptive and expressive language abilities, social communication profile, and any feeding or swallowing concerns. The report will also include recommendations for therapy frequency, setting, and areas of focus. For a closer look at how clinicians structure these reports, see our guide to slp evaluation and treatment planning.
Individualized Goal-Setting and IEP/IFSP Participation
After the evaluation, the SLP translates clinical findings into measurable goals. In school settings, these goals become part of the child's Individualized Education Program (IEP) or, for children under three, the Individualized Family Service Plan (IFSP). During team meetings, the SLP advocates for accommodations and services that match the child's communication needs, whether that means additional therapy sessions, classroom supports, or assistive technology.
Direct Therapy Delivery
Therapy sessions are designed around evidence-based practices and delivered at an intensity that supports meaningful progress.1 SLPs address areas such as:
Joint attention: Teaching the child to share focus with a communication partner.
Pragmatic language: Practicing turn-taking, topic maintenance, and understanding nonverbal cues.
Functional communication: Building reliable ways to make requests, protest, and comment, including augmentative and alternative communication (AAC) when needed.
Feeding and swallowing: Addressing oral-motor or sensory-based eating challenges when medically or educationally necessary.1
Interdisciplinary Collaboration
SLPs play a central role on the interprofessional team.1 They coordinate regularly with pediatricians, psychologists, developmental pediatricians, board-certified behavior analysts (BCBAs) who oversee ABA therapy, occupational therapists, educators, and families. To better understand how SLP vs occupational therapy roles differ and overlap, review our career comparison. This collaboration ensures that communication strategies are reinforced consistently across therapy sessions, classrooms, and home routines.
Because the scope of SLP practice with autistic children is so broad, clinicians are expected to pursue specialized education and training in autism spectrum disorder.1 If you are exploring graduate programs, look for curricula that include dedicated coursework or clinical placements focused on autism.
According to the CDC, approximately 1 in 36 children in the United States is identified with autism spectrum disorder, reflecting a prevalence of about 3.2 percent among eight year olds. Federal data collected under IDEA Part B show that speech or language impairment is one of the most common service categories for students with autism, with the majority of autistic children in public schools receiving speech-language services as part of their educational support.
Evidence-Based Speech Therapy Techniques for Autism
Choosing the right therapy approach for a child with autism is not a one-size-fits-all process. Skilled SLPs draw from a toolkit of evidence-based speech therapy techniques, selecting and combining strategies based on the child's age, verbal abilities, communication goals, and family priorities. Below are five core approaches with strong research support, along with guidance on how to evaluate any technique an SLP recommends.
Picture Exchange Communication System (PECS)
PECS teaches children to communicate by exchanging picture cards for desired items or activities. It is particularly effective for children who are minimally verbal or preverbal, giving them a structured way to initiate communication rather than waiting for prompts. Research consistently supports PECS as an evidence-based practice for building functional requesting skills, and many children who start with PECS go on to develop spoken language alongside or in place of the picture system.
NDBIs, including Enhanced Milieu Teaching (EMT), blend developmental and behavioral principles within natural, play-based contexts. Rather than drilling skills in isolation, the SLP follows the child's lead during everyday routines and uses strategies like modeling, recasting, and time delays to encourage spontaneous communication. NDBIs have a robust evidence base for toddlers and preschoolers on the spectrum, and they are especially well suited for early intervention settings where building joint attention and early language is the primary goal.
Video Modeling
Video modeling involves showing a child a short video of a peer or adult performing a target behavior, such as greeting a friend, asking for help, or taking turns in conversation. The child then practices the same skill. This technique works well for school-age children and adolescents who are visual learners, and it is supported by a strong body of evidence for teaching social communication, daily living skills, and play behaviors.
Play-Based Therapy
Play-based approaches use child-directed play as the vehicle for language learning. The SLP creates opportunities for communication during motivating activities like building with blocks, pretend cooking, or sandbox play. This method is especially effective for young children because it capitalizes on intrinsic motivation and mirrors how neurotypical language development occurs. Evidence supports play-based therapy as a way to increase vocabulary, expand sentence length, and improve social engagement.
Social Thinking and Social-Pragmatic Approaches
For children and adolescents with functional spoken language who struggle with the social use of communication, Social Thinking curricula and social-pragmatic interventions target skills like reading nonverbal cues, understanding perspectives, maintaining conversation topics, and adjusting language for different listeners. These approaches carry growing evidence support and are commonly used in school-based and group therapy settings for older children on the spectrum.
Combining Techniques for Individualized Care
In practice, SLPs rarely rely on a single technique. A preschooler who is just beginning to use words might benefit from a combination of PECS for functional requesting, EMT during snack time, and play-based therapy to build joint attention. A middle schooler might receive video modeling to learn conversational openers while also participating in a Social Thinking group. The SLP continuously assesses progress and adjusts the approach, layering strategies to match evolving needs. For clinicians interested in deepening their expertise, pursuing SLP additional certifications in areas like autism or AAC can further strengthen their clinical toolkit.
How to Evaluate the Evidence Behind a Technique
Parents and caregivers should feel empowered to ask any SLP about the research supporting a proposed technique. Two reliable resources for checking evidence ratings are ASHA's Practice Portal and the National Clearinghouse on Autism Evidence and Practice (NCAEP), both of which maintain regularly updated reviews of interventions for autistic individuals.
It is equally important to recognize that some widely marketed approaches lack scientific support. Facilitated communication, for example, involves a facilitator physically guiding a person's hand to type or point to letters. Multiple controlled studies have found that the resulting messages reflect the facilitator's influence rather than the individual's own communication, and major professional organizations, including ASHA, have issued position statements against its use. When evaluating any therapy, look for peer-reviewed research, ask about expected outcomes, and be cautious of approaches that promise dramatic results without transparent evidence.
AAC Options for Minimally Verbal Children
Augmentative and alternative communication (AAC) gives minimally verbal children on the autism spectrum a reliable way to express needs, share ideas, and build social connections. One of the most persistent myths parents encounter is that AAC will prevent or delay spoken language development. Research consistently shows the opposite: providing AAC often supports and even accelerates verbal speech because it reduces frustration and reinforces the communicative loop. The table below compares the three main AAC categories so families and future SLPs can make informed, individualized decisions.
Feature
Low-Tech (Picture Boards, PECS)
Mid-Tech (Dedicated Speech-Generating Devices)
High-Tech (Tablet-Based Apps)
Examples
Picture Exchange Communication System (PECS), picture boards, communication books, symbol cards
Dedicated single-message or sequenced-message devices (e.g., GoTalk, BIGmack)
Proloquo2Go, TouchChat, LAMP Words for Life on iPad or Android tablet
Approximate Cost Range
$0 to $300 for printed materials and binders; PECS training manuals around $50 to $200
$100 to $1,500 depending on vocabulary capacity and durability
$200 to $400 for the app plus $300 to $800 for the tablet; robust case accessories add $50 to $150
Typical Training Timeline
Families and children can begin basic exchanges within one to two weeks; full PECS protocol spans six phases over several months
Two to four weeks for basic operation; three to six months for fluent, independent use with SLP guidance
Four to eight weeks for initial navigation; six to twelve months to build robust vocabulary and sentence construction skills
Key Selection Criteria
Best for children with limited fine motor demands; no charging or tech troubleshooting required; highly portable and durable
Good for children who benefit from voice output but need a physically rugged, distraction-free device; moderate motor planning needed
Ideal for children with adequate fine motor skills and visual attention; offers large, customizable vocabulary sets; may require strategies to manage device distractions
Portability and Durability
Very lightweight and virtually indestructible; easy to carry in a backpack or attach to a wheelchair
Moderate weight; designed for drops and spills; battery life typically eight or more hours
Standard tablet weight (under two pounds with case); battery life six to ten hours; protective cases recommended for young users
Vocabulary Growth Potential
Limited by physical space; adding new symbols requires printing and organizing new cards
Moderate; vocabulary expansion depends on device model and number of programmable buttons
Extensive; apps can hold thousands of symbols, grow with the child, and support literacy development over time
Insurance and Funding Pathways
Often covered by school districts at no cost; Medicaid may reimburse PECS materials as part of therapy
Frequently covered by Medicaid and private insurance when prescribed by an SLP with a documented evaluation
Tablet-based systems may be covered when classified as dedicated speech-generating devices; school districts can also fund through assistive technology budgets
Impact on Spoken Language Development
Research shows PECS users often increase spoken word attempts during and after training
Voice output models spoken language, reinforcing verbal imitation and word learning
Robust language systems expose children to extensive vocabulary and grammar models, supporting both communication and emerging speech
Questions to Ask Yourself
Does your child communicate their needs effectively, even if they are not using spoken words?
Communication includes gestures, pictures, devices, and behavior. Recognizing all the ways your child already communicates helps the SLP build on existing strengths rather than starting from scratch.
Does the current therapy plan include goals for social communication, not just articulation?
Children on the spectrum often need support with pragmatic skills like turn-taking, reading facial expressions, and initiating conversation. A plan focused only on speech sounds may miss the areas where your child needs the most help.
Have you asked the SLP how they measure progress and when you should expect to see changes?
Clear benchmarks, such as the number of spontaneous requests per session or successful peer interactions, let you track growth objectively. Without defined milestones it is difficult to know whether to adjust the approach.
Age-Specific Therapy Approaches: Early Intervention Through Adolescence
Speech therapy for autism is not one-size-fits-all. The techniques an SLP uses, the intensity of sessions, and the goals themselves shift meaningfully as a child grows. Understanding these age bands helps families and future clinicians plan realistic, effective intervention strategies.
Birth to Age 3: Part C Early Intervention
The earliest window of opportunity is also the most powerful. Research consistently shows that intervention before age three yields the strongest documented outcomes for language development in autistic children. A Drexel University study found that among preschool-age children who received early, intensive services, roughly 66% gained single words and about 50% progressed to combining words and phrases.1
During this period, therapy is primarily parent-mediated. SLPs coach caregivers to embed communication opportunities into everyday routines such as feeding, bathing, and play. Sessions typically occur one to two times per week with the SLP, but the real therapy happens at home between visits. The focus is on building joint attention, early vocalizations, gestures, and foundational receptive language. Common approaches include naturalistic developmental behavioral interventions and, when appropriate, introduction of augmentative and alternative communication (AAC) tools.
A systematic review published through the National Center for Biotechnology Information suggests that comprehensive early intervention programs often recommend 20 or more hours per week of structured support (combining speech-language therapy with behavioral interventions) sustained over at least two years for the most meaningful gains.2
Ages 3 to 5: Preschool and Part B Services
Once a child transitions from Part C (state early intervention) to Part B (school district services) around age three, therapy often becomes more structured and group-oriented. SLPs in preschool settings focus on spoken language acquisition, play-based social communication, and early pragmatic skills like turn-taking and topic maintenance.
A JAMA Pediatrics meta-analysis on early intensive behavioral intervention (EIBI) for autism notes that children in this age range benefit from three to five sessions per week over a span of two to three years, with goals broadening to include adaptive behavior and basic conversational exchanges.3 Techniques such as the Early Start Denver Model (ESDM) blend developmental and behavioral strategies, making them well suited for preschool-age learners.
Ages 6 to 12: School-Age Support
As children enter elementary school, the therapy focus shifts from foundational language building to more complex social-pragmatic skills. SLPs work on narrative language (telling and understanding stories), inferencing, understanding figurative language, and navigating peer conversations. Session frequency often decreases compared to the preschool years, typically ranging from one to three sessions per week depending on the child's needs and the service delivery model.
School-age therapy also increasingly involves collaboration with classroom teachers and other specialists. SLPs may push into classrooms to support communication in real academic contexts rather than pulling the child into a separate therapy room for every session. Video modeling, social scripts, and structured peer interaction activities become common speech therapy techniques during this stage.
Ages 13 to 18: Adolescence and Transition Planning
The adolescent years bring a notable shift in therapy priorities. While some teens continue to work on conversational and social communication skills, SLPs also begin addressing self-advocacy, workplace communication, and the ability to navigate complex social situations such as job interviews, group projects, and community interactions.
Transition planning, which is federally required by age 16 under the Individuals with Disabilities Education Act (and earlier in some states), should include speech-language goals that support independence. Therapy at this stage tends to be less frequent, often once per week or on a consultative basis, but more targeted. Teens may participate actively in setting their own goals, which is itself a therapeutic skill.
The overarching pattern across all four age bands is clear: intervention moves from highly intensive, play-based, and parent-driven in the earliest years to increasingly self-directed and socially complex by adolescence. For students considering a career in speech-language pathology, gaining clinical experience across multiple age groups during your slp grad student schedule is one of the best ways to prepare for the diverse needs of autistic clients. Courses focused specifically on autism speech therapy techniques can deepen your understanding of how to tailor intervention to each developmental stage.
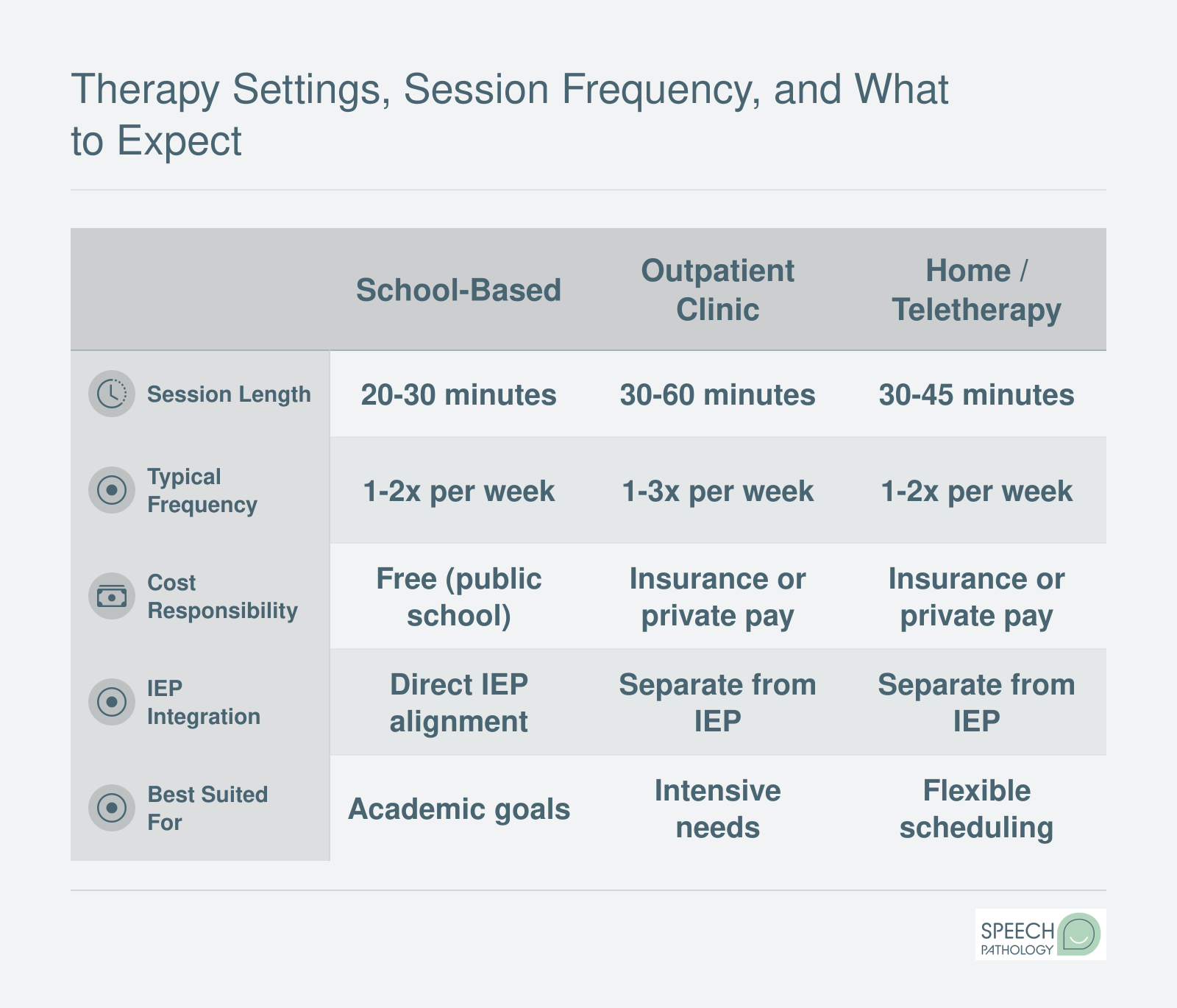
Therapy Settings, Session Frequency, and What to Expect
Speech therapy for autism can happen in several settings, and each one comes with different logistics. Understanding the basics of session length, frequency, and cost responsibility helps parents plan ahead and set realistic expectations. A typical session involves structured activities targeting individualized communication goals, often blending play, visual supports, and direct instruction.
Cost, Insurance Coverage, and Accessing Services
Understanding the financial side of autism speech therapy helps families plan ahead and avoid surprises. Costs vary widely depending on session length, provider setting, and geographic location, but several pathways exist to reduce or eliminate out-of-pocket expenses.
What Does Private-Pay Speech Therapy Cost?
For families paying out of pocket, session fees depend on duration and the provider's region. Based on current national data:
The national average hovers around $175 per session1, though costs in high-cost areas like California can climb to roughly $262 per session.6 An initial speech-language evaluation typically runs between $150 and $6004, and families who commit to a consistent therapy schedule may spend anywhere from $1,600 to $9,000 annually depending on frequency and session length.5
AAC devices add another layer of expense. A communication app on a tablet may cost a few hundred dollars, while a dedicated speech-generating device can exceed $8,000. Many insurance plans and Medicaid programs cover these devices when prescribed by an SLP, though families should expect to navigate prior authorization paperwork.
Navigating Insurance and Medicaid Coverage
All 50 states now have some form of autism insurance mandate, which is encouraging, but the details matter. Coverage caps, age limits, and the definition of "medically necessary" treatment vary significantly from state to state. Some mandates cap annual benefits at a specific dollar amount, while others impose session limits or restrict coverage to children under a certain age.
Medicaid offers an important safety net through the Early and Periodic Screening, Diagnostic and Treatment (EPSDT) benefit, which requires states to cover medically necessary speech therapy for children under 21. This includes evaluation, treatment, and AAC devices when clinically justified. Families enrolled in Medicaid should not face denials for speech therapy that an SLP has determined is needed, though appeals are sometimes necessary.
When contacting your insurance company, request a written determination of how many speech therapy sessions are covered per calendar year. Ask specifically about coverage under CPT codes 92507 (speech therapy treatment), 92508 (group treatment), and 92523 (speech-language evaluation). Having these codes on hand helps you get precise answers rather than vague assurances.
Free and Lower-Cost Alternatives
Families should know that several pathways to speech therapy carry no cost at all:
School-based services through IDEA: If a child qualifies for an Individualized Education Program (IEP), speech-language services provided at school are free to the family. The school district bears the cost.
Part C early intervention: Children from birth through age 2 who show developmental delays may qualify for early intervention services under Part C of IDEA. In many states, these services are provided at no charge regardless of family income.
University speech-language clinics: Graduate programs in speech-language pathology often operate training clinics where supervised student clinicians provide therapy at significantly reduced rates. These clinics can be an excellent option for families who need consistent, affordable care.
Your Action Step
If you are a parent exploring services, start by calling your insurance provider this week. Have your child's autism diagnosis documentation ready, reference the CPT codes listed above, and ask for a written summary of covered sessions, copay amounts, and any prior authorization requirements. If a claim is denied, request the specific reason in writing and file an appeal. State insurance commission websites often provide templates and instructions for the appeals process, and many autism advocacy organizations offer free guidance to families navigating these hurdles.
For students considering a career in speech-language pathology, understanding the financial landscape your future clients face is essential. Cost barriers directly shape how families access therapy, how consistently children attend sessions, and ultimately how much progress they make. The ability to connect families with funding resources, from insurance navigation to school-based services, is a practical clinical skill that sets effective clinicians apart. Students interested in delivering services remotely should also explore telepractice speech therapy, which can expand access for families in underserved areas.
Did You Know?
School-based speech therapy is designed to support a child's access to the educational curriculum, while private therapy can address broader social communication goals that extend beyond the classroom. Families are legally entitled to receive both types of services at the same time. If anyone suggests you must choose one or the other, know that this is not accurate. Using both together often provides the most comprehensive support for a child with autism.
How Parents Can Support Speech Therapy at Home
Therapy sessions with an SLP typically last 30 to 60 minutes, but children spend the vast majority of their waking hours at home, in the car, at the grocery store, and on the playground. That gap is exactly why parent coaching has emerged as one of the most effective evidence-based practices in pediatric speech therapy for autism. When SLPs model strategies during sessions and then equip caregivers with specific techniques to use throughout daily routines, children get hundreds of additional communication opportunities every week, and progress tends to accelerate.
If your child's SLP has not already offered structured parent coaching, ask for it. A good clinician will demonstrate a strategy in session, watch you practice it, and give you feedback before sending you home with a clear plan.
Concrete Strategies to Embed in Daily Routines
You do not need special equipment or a therapy room. The following techniques can be woven into mealtime, bathtime, play, and errands.
Narrate what you are doing: Use short, clear sentences to describe actions in real time. "I'm cutting the banana. Now I'm putting it on the plate." This saturates your child's environment with relevant language.
Use visual supports: Post a simple visual schedule for morning and bedtime routines. Point to each picture as you move through the steps so your child connects images with expectations and language.
Create communication temptations: Place a favorite snack or toy within sight but out of reach. This naturally motivates your child to request the item using words, signs, or an AAC device instead of simply grabbing it.
Follow the child's lead: If your child is lining up toy cars, sit beside them and join in rather than redirecting. Comment on what they are doing and wait. Shared attention is the foundation of social communication.
Model language one step above: If your child uses single words, respond with two-word phrases. If they say "car," you say "blue car" or "car go." This gentle expansion gives them a reachable next target without overwhelming them.
Tracking Progress at Home
Simple data collection helps you and the SLP see patterns that might otherwise go unnoticed. Consider keeping a brief daily tally of spontaneous words, signs, or AAC devices your child uses outside of therapy. Even a note on your phone works. Recording a short video once a month during the same activity (for example, snack time) creates a powerful visual comparison over several months and can highlight gains that feel invisible day to day.
At each therapy session, come prepared with a few focused questions: Which strategy is working best? Should I adjust how long I wait before prompting? Are there new targets I should practice this week?
Free and Low-Cost Materials Worth Exploring
You do not need an expensive toolkit to reinforce therapy at home. Several accessible resources can help.
Visual schedule templates: Canva offers free, customizable templates you can print at home. Boardmaker Online provides a free trial that lets you create picture-based schedules and communication boards.
AAC practice apps: Many dedicated AAC applications offer free or lite versions so families can practice using the same system at home that the SLP uses in the clinic.
Finding a qualified SLP: ASHA's ProFind directory (available on the American Speech-Language-Hearing Association website) lets you search for certified speech-language pathologists by specialty and location, which is especially helpful if you are looking for a provider experienced in autism speech therapy.
For students exploring this career path, understanding how parent coaching fits into clinical practice is essential. If you are weighing whether this field is right for you, our guide on whether speech pathology is right for you walks through the day-to-day realities of the profession.
Consistency across settings is what turns weekly therapy into real-world communication growth. When parents actively participate, children do not just practice skills in a clinical chair; they learn to use language where it matters most, in everyday life.
Frequently Asked Questions About Speech Therapy for Autism
Below are answers to some of the most common questions families and future SLPs ask about autism speech therapy. Each response draws on the evidence-based practices, therapy settings, and insurance guidance discussed throughout this article.
How many speech therapy sessions does an autistic child need per week?
Most children on the spectrum benefit from one to three sessions per week, though the ideal frequency depends on the child's age, communication level, and therapy goals. Children in early intervention or those who are minimally verbal often start on the higher end. As discussed in the therapy settings section above, an SLP will reassess session frequency at regular intervals and adjust the schedule based on measurable progress.
Does insurance cover speech therapy for autism?
Many private insurance plans, Medicaid, and CHIP programs cover speech therapy when it is deemed medically necessary. Coverage varies significantly by state and plan, so families should request a written summary of benefits and confirm whether a diagnosis of autism spectrum disorder qualifies. As noted earlier in this guide, school-based services under an IEP are provided at no cost, and families can pursue both school and private services simultaneously.
What are the best speech therapy techniques for autism?
Evidence-based techniques highlighted earlier in this article include naturalistic intervention, the Picture Exchange Communication System (PECS), video modeling, and play-based therapy. An SLP selects techniques based on the child's individual profile. For example, naturalistic intervention embeds communication practice into everyday routines, while PECS supports children who need a visual system to initiate requests and comments.
At what age should a child with autism start speech therapy?
The earlier, the better. Research consistently shows that starting speech therapy before age three, ideally through an early intervention program, leads to stronger long-term communication outcomes. However, it is never too late to begin. As outlined in the age-specific approaches section, older children and adolescents also make meaningful gains, particularly in pragmatic language and social communication skills.
How do I measure my child's speech therapy progress?
SLPs track progress through standardized assessments, language samples, goal-specific data collection, and parent or teacher questionnaires. Look for concrete indicators such as an increase in spontaneous words or phrases, more frequent use of an AAC device, or improved turn-taking during conversations. Regular progress reports, typically provided quarterly, should translate clinical data into clear milestones families can understand.
Can speech therapy help a nonverbal child learn to talk?
Yes, speech therapy can help many minimally verbal children develop spoken language, though outcomes vary. As discussed in the AAC section, SLPs often introduce augmentative and alternative communication tools (speech-generating devices, picture boards, or apps) alongside spoken language goals. Research shows that AAC does not inhibit speech development. Instead, it often serves as a bridge that supports verbal communication over time.
What is the difference between an SLP and an ABA therapist for communication goals?
An SLP specializes in the full scope of speech, language, and social communication development, including pragmatic language, articulation, and AAC. An ABA (applied behavior analysis) therapist focuses on behavior change using reinforcement strategies and may target communication as one component of a broader behavioral plan. As noted earlier, the two professionals frequently collaborate, with the SLP guiding language-specific goals while the ABA therapist reinforces those skills across settings.