Voice Therapy for Specific Conditions: Nodules, Hoarseness, Paralysis, and Transgender Voice
Voice therapy is never a one-size-fits-all process. The techniques an SLP selects, the order they introduce exercises, and the goals they set all depend on the underlying diagnosis. Below is a closer look at how therapy is tailored for four of the most common conditions that bring patients through the clinic door.
Vocal Nodules
Nodules develop when repeated vocal misuse causes callous-like growths on the vocal folds. Therapy for nodules centers on three pillars: eliminating the abusive vocal behaviors that caused the lesions, establishing resonant voice placement to reduce fold collision force, and building reliable breath support so the voice is powered from the diaphragm rather than the throat.
Research consistently shows that voice therapy alone can resolve nodules in a significant percentage of patients, particularly when the lesions are recent and the patient is committed to changing daily vocal habits. For this reason, most laryngologists recommend a trial of therapy before considering surgery. Children with nodules respond especially well because their vocal folds heal quickly once the damaging patterns stop.
Hoarseness and Muscle Tension Dysphonia
Functional dysphonia, often called muscle tension dysphonia, is one of the most frequent causes of chronic hoarseness. The vocal folds themselves may look structurally normal, yet excess tension in and around the larynx produces a strained, breathy, or rough voice quality.
Therapy targets this tension at its source. An SLP may use:
- Laryngeal massage and reposturing: Manual techniques that release the extrinsic laryngeal muscles gripping the voice box.
- Confidential voice technique: Speaking at a soft, breathy level to interrupt the cycle of effortful phonation and let the muscles reset.
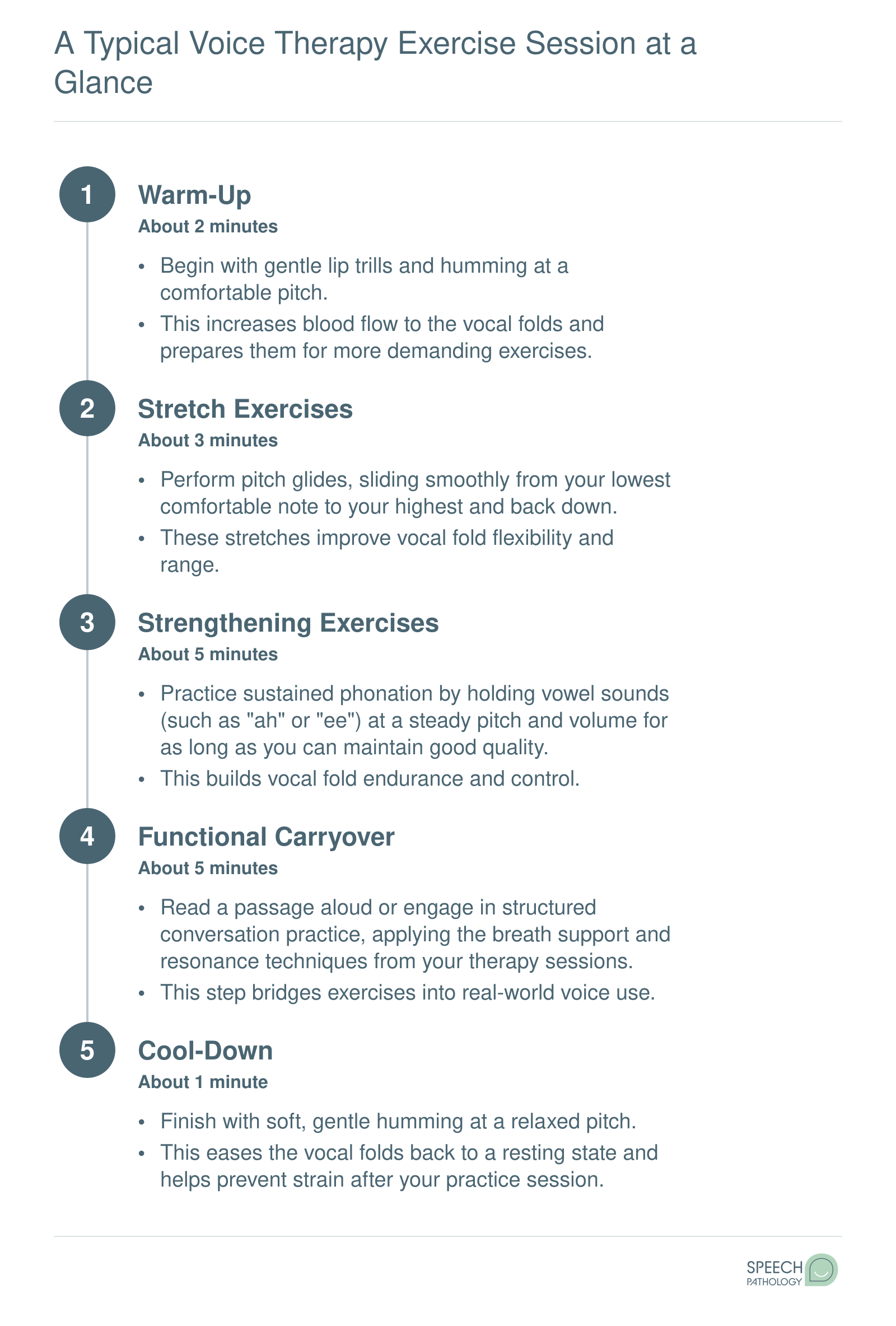
- Semi-occluded vocal tract (SOVT) exercises: Straw phonation, lip trills, and humming that create back-pressure in the vocal tract, encouraging the folds to vibrate with less effort.
Over several weeks, patients learn to replace their habitual tension patterns with easier, more efficient voicing.
Vocal Fold Paralysis
When one vocal fold is paralyzed or paretic, it cannot meet its partner at midline, leaving a gap that causes a weak, breathy voice and sometimes aspiration during swallowing. Voice therapy for paralysis focuses on improving glottal closure through compensatory strategies:
- Pushing and pulling exercises: The patient pushes down on a chair or pulls up on its seat while phonating. These effort closure techniques recruit the working fold and any residual movement in the affected fold to achieve better contact.
- Pitch manipulation: Producing voice at specific pitches that naturally bring the folds closer together.
- Head-turn technique: Turning the head toward the paralyzed side can physically shift the affected fold closer to midline, improving closure during speech.
In many cases, therapy is combined with a medical procedure such as injection laryngoplasty, where a filler material is injected into the paralyzed fold to bulk it toward the midline. The SLP then refines the patient's vocal technique around that improved anatomy.
Transgender Voice Modification
For transgender individuals, voice can be one of the most visible markers of gender presentation, and modifying it requires careful, sustained training. Therapy for transfeminine voice typically includes:
- Pitch elevation training: Gradually raising habitual speaking pitch into a target range, often using real-time visual feedback from acoustic software.
- Resonance shifting: Moving the primary resonance from the chest cavity upward into the pharynx and oral cavity, which has an even greater perceptual impact than pitch alone.
- Intonation and prosody changes: Adopting speech melody patterns, stress placement, and phrasing that align with the client's gender identity.
Transmasculine clients may also seek therapy, particularly if testosterone therapy alone does not produce the vocal quality they desire.
The timeline for transgender voice work is notably longer than for most other voice conditions, often spanning six to twelve months of consistent sessions and daily practice. Progress is incremental, and an experienced SLP helps clients set realistic milestones while protecting vocal health throughout the process.
Why a Voice-Specialized SLP Matters
Each of the conditions above demands a distinct clinical lens. Generic vocal exercises found on video-sharing platforms may seem helpful, but they miss the diagnosis-specific nuance that determines whether a technique is safe and effective for a given patient. An SLP who specializes in voice disorders brings instrumental assessment tools, condition-specific protocols, and the clinical judgment to modify exercises session by session as the voice changes. Thorough SLP evaluation and treatment planning ensures that every intervention is matched to the individual's diagnosis and goals. For students exploring this career path, voice rehabilitation is one of the most rewarding and technically precise specializations the field offers.