Points of interest…
- SLP employment is projected to grow 15 percent from 2024 to 2034.
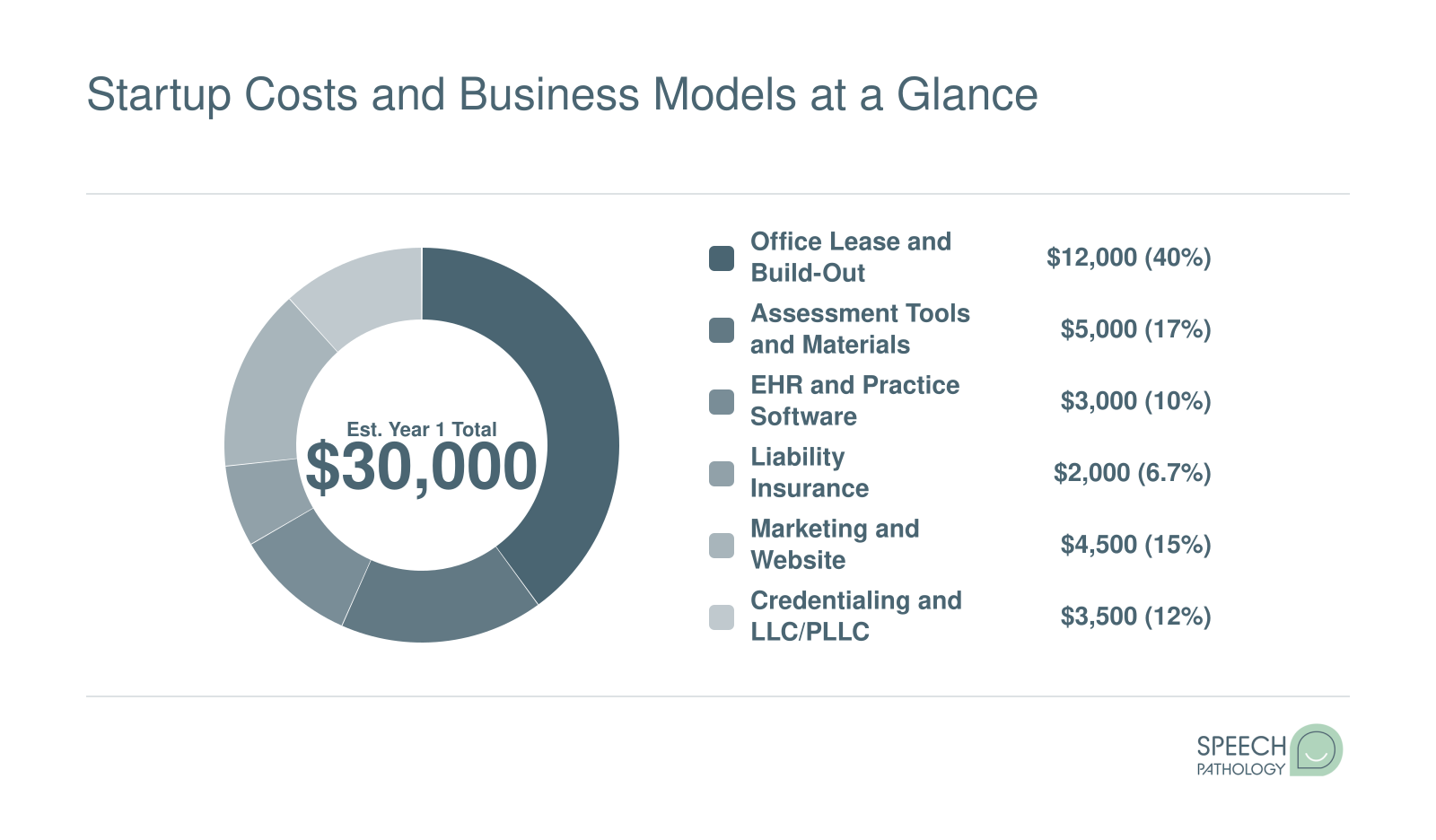
- Year one startup costs range from roughly $10,000 to over $50,000.
- Telepractice models let new practice owners launch without a physical office.

Explore the forces driving the private practice boom, what owners earn, and how rural and urban opportunities differ for speech-language pathologists.

In June 2026, Jodi Ward announced that Colorful Language Speech Therapy, PLLC would open in Emmetsburg, Iowa, a rural Palo Alto County community where access to speech-language pathology services has been limited. Her clinic, housed in a renovated storefront, is one small signal of a much larger shift: more SLPs are choosing to build private practices rather than remain in school systems, hospitals, or staffing agencies.
The reasons converge from several directions. SLP grad school burnout in institutional settings continues to push experienced clinicians toward autonomy. Telepractice has lowered the barrier to reaching clients in underserved areas. And demand for speech therapy still outpaces the supply of providers, particularly in rural counties. For SLPs weighing this path, the real tension sits between the income upside of practice ownership and the startup costs, credentialing hurdles, and business risk that come with it. Understanding CCC-SLP certification pay can help clarify exactly where the salary ceiling sits before you decide whether independence is worth the leap.
The foundation of any career trend is demand, and for speech-language pathologists, that foundation is unusually strong. According to the Bureau of Labor Statistics Occupational Outlook Handbook, the field is projected to grow 15 percent between 2024 and 2034, a rate classified as much faster than average.1 That translates to roughly 28,200 new positions over the decade and approximately 13,300 job openings every year.1 When you start from a base of about 187,400 working SLPs nationally, those numbers represent meaningful expansion, and they signal something important: the profession has enough momentum that entrepreneurial risk looks a lot more manageable than it did a generation ago.
Demand alone does not explain a private practice boom. Plenty of high-demand professions stay tethered to large employers. What is pushing SLPs out of schools, hospitals, and rehab centers is a cluster of frustrations that have been building for years.
These are not minor complaints. For many SLPs, they accumulate into a clear calculation: the trade-offs of employment no longer outweigh the trade-offs of independence.
On the other side of that calculation, several forces are making private practice more accessible than ever.
The trend is not limited to urban markets or suburban clusters. In June 2026, Jodi Ward announced the opening of Colorful Language Speech Therapy, PLLC in Emmetsburg, Iowa, a community in Palo Alto County.2 The clinic is being built out in a renovated space in town, and its arrival underscores how SLP private practice is reaching communities where institutional employers were never a realistic option in the first place. That story, reported by the Emmetsburg Reporter Democrat, is one signal among many that the movement is genuinely national in scope.
The trend, in short, is real and it is accelerating. But the first question most SLPs ask once they feel the pull is a practical one: does the money actually work?
What can you actually expect to take home as a private practice owner after overhead, taxes, and business expenses?
This question drives much of the financial planning for SLPs considering the leap from salaried positions to practice ownership. While specific income figures vary widely based on location, specialty, payer mix, and years in operation, understanding the general landscape helps set realistic expectations.
The Bureau of Labor Statistics publishes median annual wages for speech-language pathologists across employment settings. These figures provide a useful baseline, though they represent gross compensation rather than what practice owners ultimately keep. CCC-SLP salary data shows that certification level also shapes earning potential, a factor that carries over when you transition from employee to owner. Your gross revenue must cover not only your personal income but also rent, insurance, equipment, administrative costs, and potentially staff salaries.
Many new practice owners report that their first year or two involves building caseloads while managing significant startup and operational costs. Take-home pay during this early phase may fall below what you earned as a salaried clinician. However, established owners with mature practices often report earnings that exceed comparable salaried positions, particularly once overhead percentages stabilize and client volumes reach capacity.
ASHA periodically surveys private practice members and publishes findings segmented by practice characteristics, including years in operation. These surveys distinguish between gross practice revenue and net owner compensation, which is the critical number for financial planning. SLP business consultants and coaching organizations also publish case studies and aggregate data from their client bases, though access often requires membership or service enrollment.
For member-only benchmarks and candid peer discussions, consider joining ASHA's Special Interest Group focused on private practice. Members frequently share profit margins, billing rates, and operational costs in ways that generalized surveys cannot capture. Networking within these communities provides context that raw numbers alone cannot offer.
Rather than relying solely on published averages, many prospective practice owners work with CPAs or business coaches who specialize in healthcare and speech therapy practices. These professionals help you model projected income based on your specific circumstances: local reimbursement rates from insurance and private pay, anticipated client volume, and your planned service mix.
Key variables in these projections include:
SLPs who pursued a doctorate in speech-language pathology sometimes leverage that credential to command higher private-pay rates, though it is far from a requirement for practice ownership. Financial planning tools designed for SLP practices can help you stress-test different scenarios before committing to a business model.
Before you weigh the financial upside of private practice, it helps to know exactly what salaried speech-language pathologists earn in your state. The table below draws from the most recent Occupational Employment and Wage Statistics published by the U.S. Bureau of Labor Statistics (2024 data). Use these figures as your baseline: if your projected private practice revenue can meaningfully exceed the median salary in your area, the entrepreneurial leap may be worth the added risk and startup investment.
| State | Total Employed SLPs | 25th Percentile Salary | Median Salary | 75th Percentile Salary | Mean Salary |
|---|---|---|---|---|---|
| Georgia | 4,190 | $75,630 | $99,100 | $104,630 | $91,960 |
| Florida | 8,990 | $79,940 | $97,150 | $103,950 | $92,770 |
| Arizona | 2,830 | $78,680 | $95,990 | $110,330 | $98,390 |
| Virginia | 3,850 | $76,820 | $94,370 | $108,750 | $96,180 |
| Pennsylvania | 6,860 | $76,870 | $93,800 | $105,880 | $93,980 |
| South Carolina | 2,150 | $71,510 | $91,880 | $105,390 | $88,410 |
| Texas | 18,600 | $73,600 | $89,450 | $113,390 | $94,850 |
| Ohio | 7,660 | $74,300 | $88,340 | $103,500 | $89,740 |
| North Carolina | 5,160 | $69,640 | $87,420 | $102,960 | $89,980 |
| Wyoming | 270 | $67,560 | $85,820 | $107,130 | $88,930 |
| Utah | 1,450 | $62,960 | $85,320 | $102,510 | $83,640 |
| Indiana | 3,080 | $71,650 | $84,330 | $104,230 | $90,180 |
| Oklahoma | 2,040 | $62,300 | $84,310 | $106,440 | $87,210 |
| Missouri | 2,700 | $65,570 | $83,950 | $100,550 | $84,930 |
| New Hampshire | 790 | $70,350 | $83,800 | $102,710 | $86,900 |
| Tennessee | 3,510 | $65,070 | $82,990 | $100,050 | $83,200 |
| Kentucky | 2,520 | $67,140 | $82,910 | $102,190 | $86,260 |
| Illinois | 9,100 | $69,220 | $82,480 | $105,480 | $87,940 |
| Minnesota | 3,730 | $68,220 | $82,450 | $97,840 | $82,020 |
| Michigan | 4,410 | $66,550 | $81,860 | $98,740 | $84,330 |
| Nebraska | 1,230 | $67,110 | $81,710 | $98,390 | $83,880 |
| Maine | 610 | $71,440 | $81,700 | $91,660 | $80,100 |
| Kansas | 1,790 | $66,190 | $81,360 | $100,580 | $84,230 |
| Iowa | 1,390 | $73,700 | $81,120 | $98,470 | $85,230 |
| Wisconsin | 3,210 | $69,620 | $80,580 | $99,980 | $84,090 |
Watch the gap between your state's salaried SLP median and local private-pay billing rates: that spread is the clearest signal of income upside. In high-cost markets like California and New York, private-pay speech therapy sessions can exceed $200 per hour, a ceiling that salary benchmarks rarely capture.
Opening in a small Iowa town like Emmetsburg looks nothing like hanging a shingle in Denver or Boston. The rural path often means less competition but thinner referral networks and reimbursement puzzles; the urban path offers denser caseloads but crowded markets and higher overhead. Both can work. The question is which mismatch between supply and demand you want to solve.
National supply has grown from 41.4 SLPs per 100,000 residents in 2010 to 61.9 in 2024, but that headline number hides sharp regional gaps.1 The Northeast sits at 84.2 per 100,000, while the West trails at 48.2. State-level swings are wider still: Arkansas reports 101.0 SLPs per 100,000, Nevada just 33.4. In 2025, ASHA found that 55.5% of job postings exceed available job seekers, with 44.8% of funded positions going unfilled.1 An Alabama rural access study found only 35.88% of rural healthcare facilities employed an SLP in 2022, leaving large stretches of the state without local services.2
For an SLP willing to relocate or open a satellite office, that translates to steady demand, potential loan repayment programs, and warm relationships with school districts and clinics that have nowhere else to send referrals. SLPs drawn to public health career paths may find rural private practice aligns naturally with community-focused goals.
Do the homework before you commit. A few starting points:
Year 1 startup costs for an SLP private practice can range from roughly $10,000 for a solo, home-based telepractice to $50,000 or more for a brick-and-mortar clinic like the one Jodi Ward is opening in Emmetsburg, Iowa. The breakdown below reflects a mid-range estimate for a clinician launching a small in-person office. For a detailed, step-by-step walkthrough of each expense category, see the full guide on speechpathology.org.
Opening a private practice means taking on responsibilities that hospital or school employers handle for you. These challenges are solvable, but ignoring them can delay your launch by months or drain your savings before you see your first client. Understanding what lies ahead lets you plan realistically and avoid the pitfalls that derail many first-time practice owners.
Insurance credentialing is the process of becoming an in-network provider with Medicare, Medicaid, and commercial payers. It is the single biggest time sink in launching a practice, and most new owners underestimate it. The full cycle typically takes 4 to 6 months1, though it can stretch to 9 months if applications sit incomplete or payers close their panels.2
You will need to complete several steps in sequence. First, register for a National Provider Identifier (NPI), which usually takes 1 to 7 days.1 Next, create and attest your profile in the CAQH ProView system, a centralized database that payers use to verify your credentials. CAQH setup takes 1 to 2 weeks3, and you must re-attest every 120 days to keep your profile active.1 After CAQH is live, you can apply to individual payers. Medicare enrollment through PECOS takes 45 to 90 days.4 State Medicaid programs take 60 to 150 days.2 Commercial insurers (Blue Cross, Aetna, UnitedHealthcare) take 90 to 180 days, and each one requires a separate application.2 Once approved, credentialing committees review your file (2 to 4 weeks), then contracting and electronic data interchange setup adds another 1 to 3 weeks.5
The most common pitfalls are incomplete applications, missing attestations in CAQH, and waiting too long to start. If you submit an application with unsigned forms or outdated licenses, it goes to the bottom of the queue. Many payers close their panels to new providers without warning. Start credentialing 3 to 6 months before you plan to see clients6, and track every submission in a spreadsheet.
Even after you open your doors, most practices face 3 to 6 months of negative or breakeven cash flow. You cannot bill insurance until credentialing is complete, and even cash-pay clients take time to build. During this period, rent, liability insurance, electronic health record subscriptions, and marketing costs continue. Plan to have enough savings or a part-time income stream to cover both business expenses and your personal bills for at least six months.
Running a practice means managing HIPAA policies, renewing your state license, completing continuing education, and maintaining your business entity with annual filings. These are recurring costs in time and money. Solo practitioners also lose the peer support and mentorship that institutions provide. If you are weighing whether the school SLP vs. medical SLP trade-offs prepared you for independent work, that self-assessment matters here too. Joining ASHA Special Interest Group 11 (private practice) or a local SLP business network early can help you troubleshoot billing issues, share referral sources, and avoid the isolation that leads many solo owners to burn out or close within two years.
Can an SLP private practice be profitable without a physical office?
That question is no longer hypothetical. Across the profession, a growing number of speech-language pathologists are building their businesses entirely online, or blending telepractice with in-person sessions, and finding that the model opens doors that a brick-and-mortar-only clinic cannot.
For an independent clinician, every overhead dollar matters. Telepractice removes or significantly shrinks some of the largest fixed costs a new practice owner faces: commercial lease payments, utility bills, and the expense of maintaining a dedicated treatment space. When those costs drop, a solo practitioner can reach profitability with a smaller caseload, which matters a lot in the early months of building a client base.
Beyond the financial angle, telepractice speech therapy expands the geographic reach of a practice in ways that were simply not possible a decade ago. An SLP in a mid-sized city can serve clients in rural counties where no local provider exists. A clinician who relocates for personal reasons does not have to rebuild a caseload from scratch. That kind of flexibility is a genuine business asset, not just a convenience.
One of the most meaningful policy developments for telepractice entrepreneurs is the Audiology and Speech-Language Pathology Interstate Compact, commonly called the ASLP-IC. The compact is designed to let participating states streamline the licensure process so that SLPs can hold a single compact privilege and serve clients across member states, rather than applying for separate full licenses in each one.
As of 2026, the number of states that have fully enacted the compact continues to grow, though the pace of adoption varies by state legislature. Clinicians who are considering a telepractice-heavy model should check the compact's official website and ASHA's government affairs resources regularly, because the list of participating states can change within a single legislative session. Practicing across state lines without proper licensure carries real legal and professional risk, so staying current is not optional. Reviewing SLP license requirements by state is a practical first step before expanding your caseload across borders.
Many practice owners are landing on a hybrid structure: a small, low-overhead physical space for clients who benefit most from in-person interaction, combined with a robust telepractice caseload for everyone else. This approach lets the clinician keep overhead modest while still offering the hands-on sessions that certain populations, young children with complex feeding needs, for example, genuinely require.
The hybrid model also creates scheduling flexibility that full-time clinic ownership rarely allows. An SLP can see in-person clients on set days, then shift to remote sessions during hours that would otherwise go unused. For clinicians who are also juggling continuing education, consultation work, or supervision responsibilities, that kind of scheduling control is one of the most cited reasons for choosing independent practice in the first place.
Because hard, sector-wide data on telepractice revenue and adoption rates is still emerging and varies by source, prospective practice owners should do their own due diligence. ASHA's member surveys and practice data reports are a reasonable starting point for understanding how peers are using telepractice and what revenue patterns look like across different practice models. Telepractice platform providers and SLP entrepreneur communities also publish resources that can help you think through the business case before you commit.
Whether you are weighing the leap from a salaried position or mapping out your first business plan, these frequently asked questions cover the essentials. For a detailed, step-by-step walkthrough, visit the full guide at speechpathology.org.
With 15 percent projected job growth through 2034 and startup costs ranging from about $10,000 for a home-based telepractice to $50,000 or more for a brick-and-mortar clinic, the runway for new SLP practice owners is real, but it is not automatic. Success rewards those who benchmark local salaried pay against private-pay rates, budget for credentialing delays, and choose a model (rural, urban, telepractice, or hybrid) that fits their finances and lifestyle.
If this trend piece has you ready to move from curiosity to action, our step-by-step guide at /slp-private-practice/ walks through licensure, business formation, insurance paneling, and your first client pipeline. Still weighing whether private practice is the right direction entirely? Our overview of the pros and cons of being a speech pathologist can help you pressure-test the decision before you commit. The window is wide, especially in underserved communities and online, but it opens fastest for the SLPs who plan first and launch second.