A Clinical Supervisor's Guide to Giving Constructive Feedback to SLP Students
Evidence-based models, sample scripts, and practical tools for SLP clinical educators who want feedback that sticks.
By Benjamin Thompson, M.S., CCC‑SLPReviewed by SLP Editoral TeamUpdated July 13, 202625+ min read
Points of interest…
Anchor every feedback comment to specific ASHA competencies and program rubrics.
Pendleton's model and the five-step cycle prevent vague or reactive critiques.
Document written feedback from day one to support fair remediation decisions.
A clinical supervisor who relies on instinct alone and one who uses a structured feedback framework can both care deeply about their students. The difference shows up in outcomes: student retention of skills, client safety, and readiness for ASHA certification.
A recent Reddit thread in r/slp1 captured what many supervisors feel but rarely say aloud: giving feedback to SLP students is genuinely hard, and most clinicians enter supervisory roles without formal training in how to do it well. The thread drew practical responses from working SLPs, which itself signals how common the need is.
The stakes are concrete. ASHA's Council for Clinical Certification requires students to demonstrate specific competencies before earning the Certificate of Clinical Competence, and supervisors serve as the primary gatekeepers of that process. Feedback that is vague, inconsistent, or poorly timed does not just frustrate students. It delays skill development and, in client-facing settings, carries real safety implications.
Why Constructive Feedback Is Critical in SLP Clinical Education
Constructive feedback in clinical education means giving students specific, actionable information about their performance in ways that move their skills forward, rather than simply pointing out what went wrong. In speech-language pathology training, that distinction matters enormously, because the quality of feedback students receive shapes not just their confidence but the safety and effectiveness of the clients they serve.
Three Outcomes That Depend on Feedback Quality
When supervisors deliver feedback well, three things happen simultaneously. Students build the clinical skills they need to meet ASHA's certification requirements. Clients who receive services during practicum are protected, because students catch and correct errors before patterns become habits. And graduates arrive at their Clinical Fellowship ready to integrate theory, evaluate their own strengths honestly, refine their techniques, and apply ethical reasoning to complex cases. That final outcome is precisely what ASHA describes as the purpose of the Clinical Fellowship year, and it does not happen without consistent, high-quality feedback throughout the training pipeline.1
The stakes are real. ASHA's current certification standards, in effect since 2020, require students to complete SLP clinical hours requirements totaling 400 supervised hours, with supervisors providing real-time oversight throughout.1 Supervisors themselves must hold the CCC-SLP and have at least nine months of professional experience. They are also expected to complete at least two hours of professional development specifically focused on supervision, covering topics such as collaborative supervision models, adult learning principles, ethics, and roles and responsibilities.2 These are not administrative checkboxes; they signal that ASHA treats supervision as a distinct clinical skill with its own learning curve.
Constructive vs. Corrective: A Crucial Distinction
Purely corrective feedback tells a student what was wrong. Constructive feedback does that and then connects the error to an explanation, models an alternative, and invites the student to problem-solve. The goal is behavior change that the student owns, not compliance that evaporates the moment the supervisor leaves the room. This distinction matters especially as students approach graduation, because a clinician who understands why something went wrong is far more prepared for independent practice than one who simply learned what not to do.
Surveys of graduate students consistently identify poor or absent supervisor feedback as one of the top reasons they rate a clinical placement negatively. When feedback is vague, delayed, or withheld to avoid conflict, students lose the opportunity to course-correct, and problems that could have been addressed early become the basis for remediation or, in serious cases, a failing evaluation.
Matching Feedback to the Student's Training Stage
Not all students need the same kind of feedback. Early practicum students are still developing foundational clinical reasoning and often benefit from more directive guidance: clear identification of what happened, why it matters, and a concrete suggestion for next time. Students in final externship placements, by contrast, are preparing for independent practice and respond better to collaborative feedback models that ask them to reflect first, identify their own gaps, and co-construct solutions with their supervisor.
ASHA's CFCC has flagged competency-based standards and expanded telesupervision frameworks as strategic priorities,3 and the next revision of certification standards is expected to take effect in 2027.4 As those updates move through peer review, supervisors who already align their feedback practices to competency-based thinking will be well positioned to meet whatever new expectations emerge.
Proven Feedback Models for SLP Supervisors
No single feedback model fits every student, every placement, or every moment in a session debrief. Clinical supervisors in speech-language pathology now have access to a growing body of evidence from health professions education that can sharpen how feedback lands and how students grow from it.
Pendleton's Rules: Start with the Student
Pendleton's Rules flip the traditional script by putting the learner in the driver's seat first. The sequence moves through four steps: the student reflects on what went well, the supervisor reinforces those positives, the student identifies what they would do differently, and then the supervisor adds their own suggestions.1 This structure creates a genuinely safer space for discussing errors, because the student has already named the problem before the supervisor does.
Research across health professions education consistently describes Pendleton's Rules as less educator-centred than models where the supervisor leads with their own observations.1 That shift in ownership matters. When a first-year graduate student in a university clinic hears her own assessment of a stuttering treatment session before her supervisor comments, she is more likely to internalize the correction than if the feedback arrives top-down. The model also carries broad applicability across teaching and workplace settings beyond clinical medicine.4
Use this when: you are providing end-of-session or end-of-week macro-feedback and you want the student to build genuine self-monitoring habits rather than simply comply with your direction.
The Feedback Sandwich: Useful, But Handle with Care
The feedback sandwich, positive-corrective-positive, is probably the most widely recognized model in clinical education, partly because it is intuitive and partly because it feels kind. It works reasonably well with students who have very low insight or who are early enough in training that they need the corrective message wrapped in something reassuring.1
The well-documented risk, though, is that students remember the praise and skim the correction. If a debrief focuses mostly on encouraging framing, the critical message can create a false-positive impression of performance.1 Research comparing structured dialogic approaches suggests the feedback sandwich is less effective than methods that keep the student actively engaged in self-assessment.2 In clinical settings where a student needs to change specific behaviors before an upcoming competency evaluation, that blurring can cause real harm to both the student and their clients.
Use this when: a student is in early placement, is particularly anxious, and needs scaffolding before they can process direct critique. Pair it with a clear verbal summary of the single most important corrective point so it does not get lost.
Anderson's Continuum: Matching Supervision to Stage
Jean Anderson's Continuum of Supervision describes a developmental arc with three phases: evaluation-feedback (the supervisor is highly directive and provides frequent structured input), transitional (the supervisor and student share responsibility for identifying goals and problems), and consultative (the student drives the process and the supervisor functions more as a peer consultant).
This model maps naturally to the progression from first SLP clinical placements through externship. A second-semester graduate student in a hospital acute care rotation needs something much closer to the evaluation-feedback end of the continuum. A student completing their final externship who is eight weeks from graduation needs the supervisor to step back and consult rather than direct.
Use this when: you are onboarding a student at the start of a new placement. Locating where they fall on the continuum first tells you how much scaffolding to provide and how much autonomy to extend.
Collaborative and Proactive Solutions for Students Who Push Back
Some students struggle with traditional top-down feedback regardless of how thoughtfully it is delivered. They may become defensive, shut down, or cycle through the same errors without apparent progress. Collaborative and Proactive Solutions, a framework developed by Ross Greene for working with children who have behavioral challenges, has been adapted in clinical education contexts to address exactly this pattern.
The core idea is that unsolved problems between supervisor and student are approached collaboratively rather than correctively. Instead of the supervisor presenting the problem and the solution, both parties work together to define the obstacle and brainstorm realistic fixes. This approach is particularly useful when a student's difficulty seems rooted in anxiety, prior negative supervision experiences, or a mismatch between learning style and supervision style.
Use this when: standard structured feedback is not producing behavioral change, when a student appears to understand the correction but cannot implement it, or when the supervisory relationship itself feels strained.
A 5-Step Process for Delivering Constructive Feedback to SLP Students
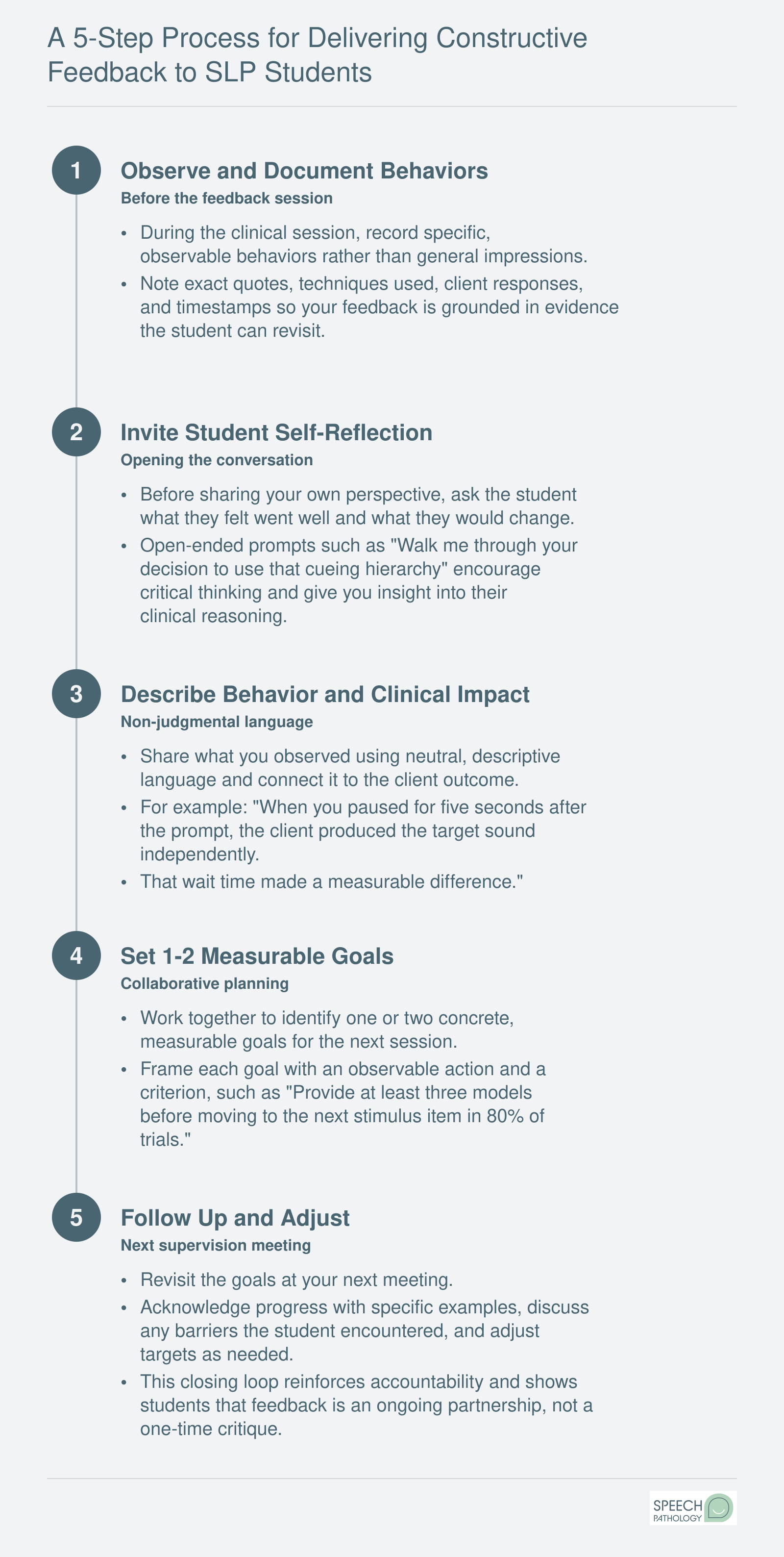
Effective clinical feedback is not a single conversation. It is a repeatable cycle that begins with careful observation and ends with collaborative goal setting and follow-through. Use this five-step process each time you sit down with an SLP student to discuss their clinical performance.
Questions to Ask Yourself
Am I giving directive correction to a student who is ready for collaborative problem-solving?
A student in their final placement who receives only prescriptive feedback misses the chance to build clinical reasoning. Over-directing an advanced student can undermine the confidence they will need as an independent clinician.
Do I adjust the ratio of positive-to-corrective feedback based on whether this is Week 2 or Week 12?
Early in a placement, heavier positive reinforcement builds the foundation students need to take risks. By Week 12, a higher proportion of corrective feedback better mirrors the accountability expectations of professional practice.
Have I asked this student how they prefer to receive feedback?
Some students process critique better in writing before a verbal debrief; others need the conversation first. Skipping this question risks delivering feedback in a format that creates defensiveness rather than growth.
Sample Scripts and Phrases for Common Supervision Scenarios
Choosing the right words during a feedback conversation can make the difference between a student who shuts down and one who grows. The table below pairs common supervision scenarios with examples of ineffective phrasing, a constructive alternative, and a brief explanation of why the reframed language works. Use these scripts as starting points, then adapt them to your own voice and your student's learning stage.
Scenario
Ineffective Phrasing
Constructive Alternative
Why It Works
Student struggles with treatment fidelity
"You keep doing the activity wrong."
"I noticed the target was presented inconsistently during the last three trials. Let's look at the session recording together and identify where adjustments would strengthen fidelity."
Anchors feedback to observable behavior and invites collaborative problem solving rather than labeling the student.
Student has difficulty building rapport with a client
"You're not connecting with this client at all."
"The client seemed quieter today than usual. What do you think might help them feel more comfortable? I have a couple of ideas we could try next session."
Opens a dialogue, normalizes the challenge, and positions the supervisor as a partner instead of a critic.
Student's documentation is below expectations
"Your SOAP notes are really bad."
"Your subjective and objective sections are solid. The assessment section needs more clinical reasoning to connect the data to your goals. Here is an example of what that analysis could look like."
Recognizes existing strengths, specifies the gap, and provides a concrete model the student can follow.
Student becomes defensive when receiving feedback
"You need to stop taking everything so personally."
"I can see this feedback feels frustrating. My goal is to help you succeed. Can we take a moment and then talk about one or two priorities for next week?"
Validates the student's emotional response, reaffirms the purpose of feedback, and narrows the focus to actionable next steps.
Student is consistently late to sessions
"You're being unprofessional by showing up late."
"Punctuality is part of the professional expectations outlined in our supervision contract. You have been late to three of the last five sessions. Let's discuss what barriers you are facing and create a plan to address them."
References a shared agreement, states observable facts without character judgment, and shifts toward solutions.
Student overestimates own clinical skills
"You think you're better at this than you actually are."
"Your self-rating on fluency intervention was higher than what I observed during today's session. Let's compare your self-evaluation with the rubric criteria so we can calibrate together."
Uses data (self-rating versus observed performance) to guide self-reflection rather than undermining the student's confidence.
Student needs to improve cueing hierarchy use
"You gave the client the answer every time."
"I noticed you moved to a direct model after the first attempt. What would happen if you tried a phonemic cue or a semantic cue before modeling? Let's practice that sequence before your next session."
Describes the specific behavior, introduces clinical reasoning through a question, and offers a chance to rehearse the skill.
Mapping Feedback to ASHA Competencies and Program Rubrics
Feedback that references a specific ASHA standard is harder to argue with than feedback that reflects a supervisor's personal preference. When you anchor observations to the Council for Clinical Certification (CFCC) Standard V clinical competencies, you shift the conversation from "I didn't like how you did that" to "Here is the competency you need to demonstrate, and here is what I observed." That framing protects the student, protects you, and makes the feedback teachable.
Why Standard V Anchoring Matters
The 2020 SLP Certification Standards require students to complete 400 clinical hours (25 observation, 375 direct client contact), with at least 25% direct supervision of every session and a minimum of 60 minutes of supervised activity for any session to count.1 Standard V specifies that competency is verified through ongoing performance evaluation across the lifespan, across disorder areas, and across assessment, intervention, and counseling activities.2 In other words, ASHA already expects you to be evaluating skills continuously, not just at midterm and finals. Tying each piece of feedback to a Standard V sub-competency makes that ongoing evaluation visible and defensible.
A Practical Observation-to-Feedback Workflow
Use a three-step loop after each session:
Observe the behavior: Note the specific action, for example, "student did not adjust cueing hierarchy when client produced three consecutive errors."
Identify the competency: Map it to the relevant Standard V clinical skill area, such as intervention decision-making or ongoing data-based clinical judgment.
Write the feedback against the rubric criterion: "On the intervention adaptation criterion, you're currently performing at a 2 (requires prompting). To reach a 3 (independent with minor adjustment), try reducing your cue level after two consecutive correct responses."
Rubrics as the Bridge
Program evaluation tools translate ASHA standards into daily language. CALIPSO, the most widely adopted platform, lets supervisors track hours, document supervision percentages, and record competency ratings tied directly to CFCC categories.1 Custom program rubrics do the same job on paper. Either way, the rubric is the bridge between what ASHA requires and what you say to a student on a Tuesday afternoon. SLP evaluation and treatment planning resources can help you connect those rubric criteria to real session goals.
Document After Every Session
Write the competency-mapped feedback down, in CALIPSO or your program's system, the same day. A verbal debrief is not a record. If remediation later becomes necessary, the paper trail of dated, standard-referenced observations is what makes a fail decision defensible. Two supervisor professional development hours per certification cycle is the minimum ASHA expects;1 documentation habits are where those hours pay off.
Build a paper trail from day one. Routine written feedback after every session or week protects both you and your student. If remediation becomes necessary, a pattern of documented concerns and support strategies is essential for defensible decisions and fair due process. Waiting until a crisis point leaves both parties vulnerable.
Handling Difficult Situations: Remediation, Documentation, and Pass/fail Decisions
When repeated clinical feedback fails to change a student's behavior, the supervisor's role shifts from coach to gatekeeper of professional standards. Knowing how to handle remediation, documentation, and pass/fail decisions protects both the student's rights and the integrity of the program.
Distinguishing Coaching From Formal Remediation
Not every struggling student needs a remediation plan. Some simply require more time and practice to develop clinical skills, such as managing fluency disorders or administering bedside swallows. Remediation is warranted when a student repeatedly fails to implement targeted feedback despite direct instruction, modeling, and multiple opportunities to improve. Look for patterns: the same error recurs across several sessions, the student cannot articulate what they will do differently, or their behavior suggests disregard for supervisory guidance. These red flags indicate that informal coaching is not sufficient.
Components of an Effective Remediation Plan
A formal remediation plan must be clear, measurable, and time-bound. Start by identifying specific deficit behaviors with objective evidence1, such as 'writes SOAP notes that lack measurable goals' or 'interrupts patients during interviews.' Then set concrete, observable goals: 'will independently write three SOAP notes with measurable goals approved by the supervisor by October 15.' Include a realistic timeline, typically two to four weeks, and list resources such as additional observation hours, peer modeling, or targeted practice modules. Specify the consequences of non-improvement, which may include a failing grade for the practicum or dismissal from the program. Many accredited SLP programs, including those at Kean University2 and St. John's University3, use a written remediation contract signed by the student, supervisor, and clinical director. Buffalo State's consultation report form serves a similar formalizing function.4 These documents become part of the student's permanent record.
Documentation That Stands Up to Scrutiny
Thorough documentation is your first defense. Record every feedback conversation with the date, the specific issue discussed, the plan for improvement, and the student's response. Keep language factual and avoid interpretation: 'student arrived 15 minutes late and did not have materials prepared' rather than 'student is unprofessional.' Ask the student to sign each entry to acknowledge they have received the feedback. Involve the graduate program director or clinical education coordinator early, particularly if you suspect the student may need accommodations under the ADA. Due process means the student must know exactly what is expected, have a reasonable chance to meet those expectations, and understand the consequences of not doing so.1 Program handbooks typically outline these procedures, and following them to the letter protects you and the institution from legal challenge.
Making the Pass/Fail Decision
Deciding to fail a student is never easy, but it is sometimes necessary to uphold ASHA competency standards for clinical education. The decision should never be made unilaterally. Consult with the clinical supervisor team, academic advisor, and program director to ensure the decision is fair and consistent with program policy. If the remediation period ends without sufficient progress, schedule a meeting with the student to deliver the outcome. Refer to the documented evidence: 'Based on the goals we set on September 1, these competencies have not been met.' Be direct yet compassionate; avoid couching the message in false hope. Provide information about any appeal process and offer to discuss next steps, whether that means retaking the practicum or exploring SLP internship and externship options. A clear, well-documented process helps the student accept the outcome and preserves their dignity.
Adapting Feedback for Telepractice and Hybrid Placements
Live telepractice observation counts as direct supervision under current ASHA guidelines,1 and asynchronous video review is treated as indirect supervision, meaning clinical educators can build a complete feedback workflow around remote tools without sacrificing compliance. That said, telepractice and hybrid placements introduce friction that supervisors must plan around.
Unique Challenges of Remote Supervision
When you observe a student through a screen, you lose access to many of the nonverbal cues that guide in-person feedback: body positioning relative to the client, the energy in the room, subtle shifts in a child's attention. Technology adds its own layer of interference. A laggy connection can make it hard to tell whether a pause was intentional wait time or a moment of uncertainty. Asynchronous timing compounds the issue further, because feedback delivered hours or days after a session lacks the immediacy that helps students connect your comments to specific clinical moments.
Recognizing these limitations is the first step. The second is choosing tools and workflows that compensate for them.
Asynchronous Video Review With Timestamped Annotations
One of the most effective strategies is having the student record a session and submit it for annotated review. Platforms such as GoReact are designed for exactly this purpose: supervisors can drop timestamped comments at precise moments in the video, and students can respond to each annotation in a threaded conversation. This approach lets you be highly specific ("At 4:32, notice the client's eye gaze shifted; that was an ideal moment to model the target phrase") without relying on memory. For quick, informal video walkthroughs, tools like Loom allow you to record a screencast of yourself watching the student's session and narrating your observations, though you will need to confirm that any platform you use meets HIPAA and FERPA compliance requirements.2
Real-Time Cueing During Live Sessions
During synchronous telepractice sessions, screen-sharing annotations and private chat channels give supervisors a way to cue students without disrupting the client interaction. You might type a brief prompt in a chat sidebar ("Try an open-ended question here") or use a pre-arranged visual signal, such as a colored icon in the corner of the screen. Platforms built for telehealth, including Doxy.me, VSee, TheraPlatform, and Zoom for Healthcare, offer the encrypted connections and audit trails that SLP telepractice guidelines require.2 Whichever platform you choose, confirm it supports secure, encrypted software with adequate bandwidth to avoid the kind of audio or video dropouts that undermine both therapy and supervision.
Compliance and Continuing Education
ASHA's Telepractice Practice Portal specifies that telepractice supervision must be equivalent in quality to in-person supervision, and all sessions must be documented.1 Beyond federal privacy requirements, supervisors should verify state licensure rules and payer-specific policies, which can vary significantly.3 ASHA also offers continuing education courses focused on telepractice and telesupervision ethics,4 which are worth pursuing if remote placements are a regular part of your supervisory load.
A few practical recommendations to keep your telepractice feedback workflow running smoothly:
Set expectations early: Outline which sessions will be observed live versus recorded, and specify turnaround times for asynchronous feedback.
Use a consistent platform: Switching between tools creates confusion; pick one HIPAA-compliant system and build your rubrics around its features.
Supplement with brief check-ins: A five-minute video call after a recorded session review can restore the conversational tone that written annotations sometimes lack.
Archive everything: Telepractice documentation requirements are explicit, so save annotated videos, chat logs, and written feedback summaries in a secure, organized location.
Remote supervision is no longer an exception. It is a standard part of clinical placements in speech-language pathology. The supervisors who adapt their feedback methods to fit this reality, rather than treating it as a lesser version of in-person observation, will give their students a stronger foundation for the telepractice caseloads many of them will eventually carry.
Quick-Reference: Feedback Approach by Student Stage
Effective clinical supervision means recognizing that a student in their first practicum needs a fundamentally different feedback approach than one completing a final externship. Tailoring your strategy to each developmental stage helps students build confidence while meeting clinical competencies. The following breakdown summarizes evidence-informed approaches for each phase of clinical education.
Early Practicum Students
Students just beginning their clinical experiences benefit most from formative assessment strategies. At this stage, the goal is not summative evaluation but ongoing guidance that shapes skill development in real time. Research on feedback in workplace-based learning suggests that establishing trust and communicating clear standards early on improves student receptiveness to feedback.1
Focus on: Building foundational skills, understanding clinic routines, and developing self-reflection habits.
Feedback style: Frequent, specific, and encouraging. Use concrete examples and model the behaviors you want to see.
Tip: Frame corrections as learning opportunities rather than deficits. Early positive experiences with feedback encourage students to seek it out proactively throughout their training.1
Mid-Placement Students
Once students have their footing, feedback can shift toward standards-based evaluation across multiple clinical episodes. Research on work-integrated learning finds that students at this stage respond well to feedback that references specific competency benchmarks and tracks progress over time.1 SLP clinical placements in grad school often mark this transition, when supervisors can invite more analytical self-evaluation before sharing their own observations.
Focus on: Connecting discrete skills to broader clinical reasoning, increasing independence, and refining self-assessment accuracy.
Feedback style: More direct and analytical. Invite students to self-evaluate before you share your observations.
Tip: Students who actively seek feedback at this stage tend to show stronger outcomes.2 Encourage questions and collaborative problem-solving.
Final Externship Students
Students nearing the end of their SLP externships are preparing to practice independently. Feedback research indicates that a relational, supportive tone at this stage correlates with both improved confidence and better acceptance of constructive criticism.3 These students are often highly attuned to how feedback is delivered.
Focus on: Professional identity, autonomous decision-making, and readiness for entry-level practice.
Feedback style: Collegial and future-oriented. Discuss clinical choices as you would with a junior colleague, while still holding students accountable to standards.
Tip: Acknowledge growth and competence explicitly. Students who feel respected and supported are more likely to internalize feedback and translate it into lasting professional habits.4
Matching your feedback approach to the student's developmental stage is not about lowering expectations for early learners or withholding guidance from advanced students. It is about meeting each student where they are so your feedback can have the greatest impact on their clinical growth.
Creating a Psychologically Safe Supervision Environment
Why does feedback feel threatening to some students and energizing to others? The difference often lies in psychological safety: the learner's confidence that they can take interpersonal risks, make mistakes, ask questions, and share uncertainty without fear of punishment, humiliation, or damage to their standing. In the supervisor-student context, psychological safety is the foundation that determines whether corrective feedback leads to growth or defensiveness. When students trust that feedback is intended to support their development rather than to judge them, they absorb it more deeply, implement it more consistently, and engage more openly in reflective practice.
Normalizing Discomfort and Modeling Emotional Regulation
Receiving corrective feedback is inherently uncomfortable. Even confident students experience a physiological stress response when a supervisor points out an error in session management or a deficit in diagnostic reasoning. Effective supervisors acknowledge this reality explicitly at the start of the placement: "You will hear feedback that feels uncomfortable. That discomfort is a sign that you are stretching, not a sign that you are failing." Model how to process feedback by thinking aloud when you receive it yourself, whether from a colleague, a parent, or a student. Share how you distinguish between feedback that calls for immediate action and feedback that requires reflection. This normalization reduces shame and reframes corrective input as a routine part of professional life. For students working to develop this resilience earlier in their training, building confidence in SLP clinical placements offers practical strategies they can draw on before supervision even begins.
Addressing Cultural and Linguistic Identity Dynamics
Supervisor-student identity dynamics, including race, language background, gender, and age, shape how feedback is perceived and delivered. A supervisor from a dominant cultural group may underestimate the cumulative weight of repeated correction for a student who is already navigating stereotype threat or code-switching demands in the clinic. Conversely, a student may interpret direct feedback as harsher than intended if their cultural norms favor indirect communication. Supervisors must reflect on their own identity and communication style, seek supervision of supervision when dynamics feel strained, and invite students to share how they prefer to receive feedback. Ask early in the placement: "What has worked well for you in past feedback conversations? What has not worked?"
Four Concrete Practices to Build Safety
Establish a feedback contract at the start of placement: Co-create expectations around timing (e.g., debrief within 30 minutes of a session), format (written, verbal, or both), and student preferences. Revisit the contract at midterm.
Use consistent structure for feedback conversations: Open with observation, invite the student's self-assessment, offer your perspective, agree on one or two action steps, and close with affirmation. Predictability reduces anxiety.
Separate feedback on clinical skills from feedback on professional behavior: Address time management, communication with staff, and adherence to clinic policies in distinct conversations from clinical decision-making. Conflating the two can obscure what the student needs to prioritize.
Check in regularly on the supervisory relationship itself: At midterm and again three weeks before the placement ends, ask: "How is this supervision working for you? What do you need more or less of from me?" This meta-conversation signals that the relationship is collaborative, not authoritarian, and gives students permission to request adjustments before resentment builds.
Questions to Ask Yourself
Does the student initiate questions or only respond when asked?
Students who only answer direct questions may be uncertain whether their input is welcome. Proactive question-asking signals comfort with the supervisory relationship and genuine investment in learning.
Has the student ever disagreed with your feedback and felt safe doing so?
Respectful disagreement indicates psychological safety. If students never push back or offer alternative perspectives, they may be suppressing concerns that could affect their clinical growth and confidence.
When was the last time you explicitly asked how the supervisory relationship is going?
Regular check-ins about the relationship itself uncover friction before it becomes a barrier. Waiting for problems to surface on their own often means waiting too long.
Frequently Asked Questions About SLP Student Feedback
Clinical supervisors often share similar questions about how to deliver feedback effectively, maintain student morale, and stay aligned with professional standards. Below are answers to the most common concerns, with pointers to the relevant sections of this guide for a deeper dive.
What are the 5 steps to giving constructive feedback?
A reliable five-step process includes: (1) observe and collect specific evidence, (2) open the conversation by inviting the student's self-reflection, (3) share your observations using objective, behavior-focused language, (4) collaborate on an action plan with measurable goals, and (5) follow up in a defined timeframe. The infographic section of this article walks through each step in detail.
How do you give constructive feedback to a student clinician without discouraging them?
Start by asking the student what they felt went well, then anchor your feedback to observable behaviors rather than character traits. Pair each area for growth with a concrete strategy the student can try immediately. Normalizing the learning curve and acknowledging effort helps maintain motivation. The section on creating a psychologically safe supervision environment covers this in greater depth.
What should an SLP supervisor do when a student does not respond to feedback?
First, confirm the student understands the feedback by asking them to restate the concern and the expected change. If progress stalls, increase the frequency and specificity of feedback sessions, involve the university's clinical coordinator, and begin formal documentation. The section on remediation, documentation, and pass/fail decisions outlines a step-by-step escalation process.
How do you document feedback and remediation for an SLP student?
Keep written records of every feedback session, including the date, behaviors discussed, agreed-upon action steps, and deadlines. Use your program's official rubrics and, when remediation is needed, create a written improvement plan signed by both parties. The callout on documenting before you need to and the remediation section offer templates and best practices.
How should feedback be adapted for telepractice SLP supervision?
In virtual settings, schedule dedicated video check-ins rather than relying solely on chat or email, since tone can be lost in text. Use screen-sharing to review session recordings together, and provide written summaries after each conversation so nothing is misinterpreted. The section on adapting feedback for telepractice and hybrid placements addresses platform-specific strategies and timing considerations.
What are the best feedback techniques for SLP clinical supervisors?
Evidence-based approaches include Pendleton's rules, the feedback sandwich, and reflective questioning models. The most effective supervisors match their technique to the student's developmental stage, moving from more directive methods early in a placement to collaborative and consultative styles as competence grows. The section on proven feedback models compares these approaches side by side.