The 4 Types of Lisps Explained
Not all lisps sound the same, and knowing which type a child or adult presents with is the first step toward effective treatment. Speech-language pathologists classify lisps into four distinct categories based on where the tongue sits and how airflow is directed during sibilant sounds like /s/ and /z/. Lisping is one of the most recognizable speech-language disorders, so understanding its subtypes helps clinicians and parents choose the right path forward.
Interdental (Frontal) Lisp
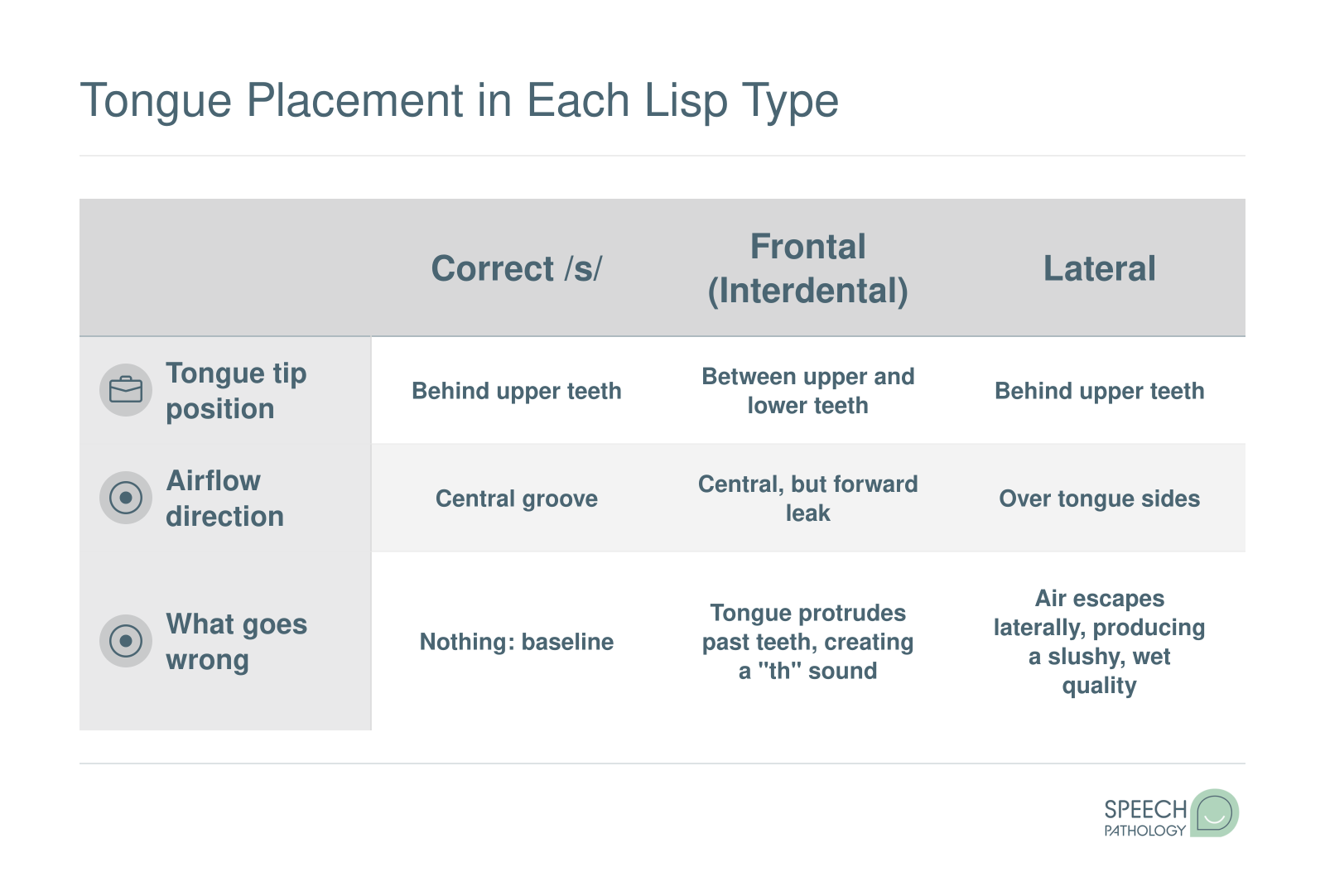
In an interdental lisp, the tongue pushes forward between the upper and lower front teeth when producing /s/ and /z/. This placement redirects airflow and turns crisp sibilants into sounds that closely resemble "th." A child with an interdental lisp might say "thun" instead of "sun" or "thoo" instead of "zoo."
You will sometimes see this called a frontal lisp. The two terms are interchangeable, and both describe the same forward tongue posture. If you encounter different labels across websites or in a therapist's notes, rest assured they refer to the same pattern.
Interdental lisps are developmentally common in young children. Many kids naturally outgrow them by age four and a half to five as their oral-motor coordination matures.
Lateral Lisp
A lateral lisp occurs when air escapes over the sides of the tongue rather than flowing in a narrow stream down the center. The result is a wet, "slushy" quality that can make words like "soup" or "see" sound distorted and muffled. Parents sometimes describe it as a sound that seems "too wet" or messy compared to a typical /s/.
Unlike the interdental variety, a lateral lisp is not considered a normal part of speech development. It rarely self-corrects and almost always requires direct intervention from a speech-language pathologist.
Dentalized Lisp
A dentalized lisp is closely related to the interdental type, but the tongue does not actually protrude between the teeth. Instead, it pushes firmly against the back of the upper front teeth. The airflow is disrupted just enough to produce a slightly dull or muffled /s/, though the distortion is often subtler than what you hear with an interdental lisp. A word like "see" may sound flat rather than sharp, without the obvious "th" substitution.
Palatal Lisp
In a palatal lisp, the middle portion of the tongue rises and contacts the hard palate (the roof of the mouth) during sibilant production. Because the tongue is positioned too far back, the resulting sound has a heavy, almost "gushy" quality. A word like "sip" can sound noticeably different, though the specific distortion is harder for untrained listeners to pinpoint compared to the more recognizable interdental pattern.
The Most Common Point of Confusion: Lateral vs. Interdental
The single question parents ask most often is: what is the difference between a lateral lisp and an interdental lisp? The answer comes down to where the air goes.
- Interdental lisp: Air flows forward over the tongue tip, which protrudes between the front teeth. The sound mimics "th."
- Lateral lisp: Air spills over the sides of the tongue, creating a wet, slushy distortion with no "th" quality.
This distinction matters enormously for prognosis. An interdental lisp in a three-year-old is generally not a cause for alarm because many children resolve it on their own as part of typical development. A lateral lisp at any age, however, is a strong signal that professional evaluation is warranted. Because it falls outside normal developmental patterns, waiting and hoping it will disappear on its own can delay progress that evidence-based speech therapy techniques could achieve much sooner.
If you are unsure which type your child or client presents with, a certified speech-language pathologist can conduct a thorough assessment and pinpoint the specific error pattern, setting the stage for an individualized treatment plan.