How SLPs Assess and Recommend AAC Solutions
Selecting the right AAC device is not a quick recommendation. It is a structured clinical process that unfolds over weeks and involves multiple professionals. Speech-language pathologists lead this process, but the best outcomes come from collaboration and careful evaluation. Understanding how the assessment works can help future SLPs prepare for one of the most impactful services they will provide.
The SETT Framework: A Standard Assessment Model
Most AAC assessments follow the SETT framework, developed by Joy Zabala, which stands for Student, Environment, Tasks, and Tools. Rather than jumping straight to a device, the SLP first evaluates the individual's current communication abilities, physical and cognitive strengths, and the settings where communication needs to happen. From there, the clinician identifies the specific tasks the person needs to accomplish, such as requesting items, participating in class discussions, or managing social interactions. Only after analyzing these three factors does the team consider which tools are the best fit. This approach prevents the common mistake of choosing technology first and forcing the user to adapt to it.
Referral, Feature Matching, and Device Trials
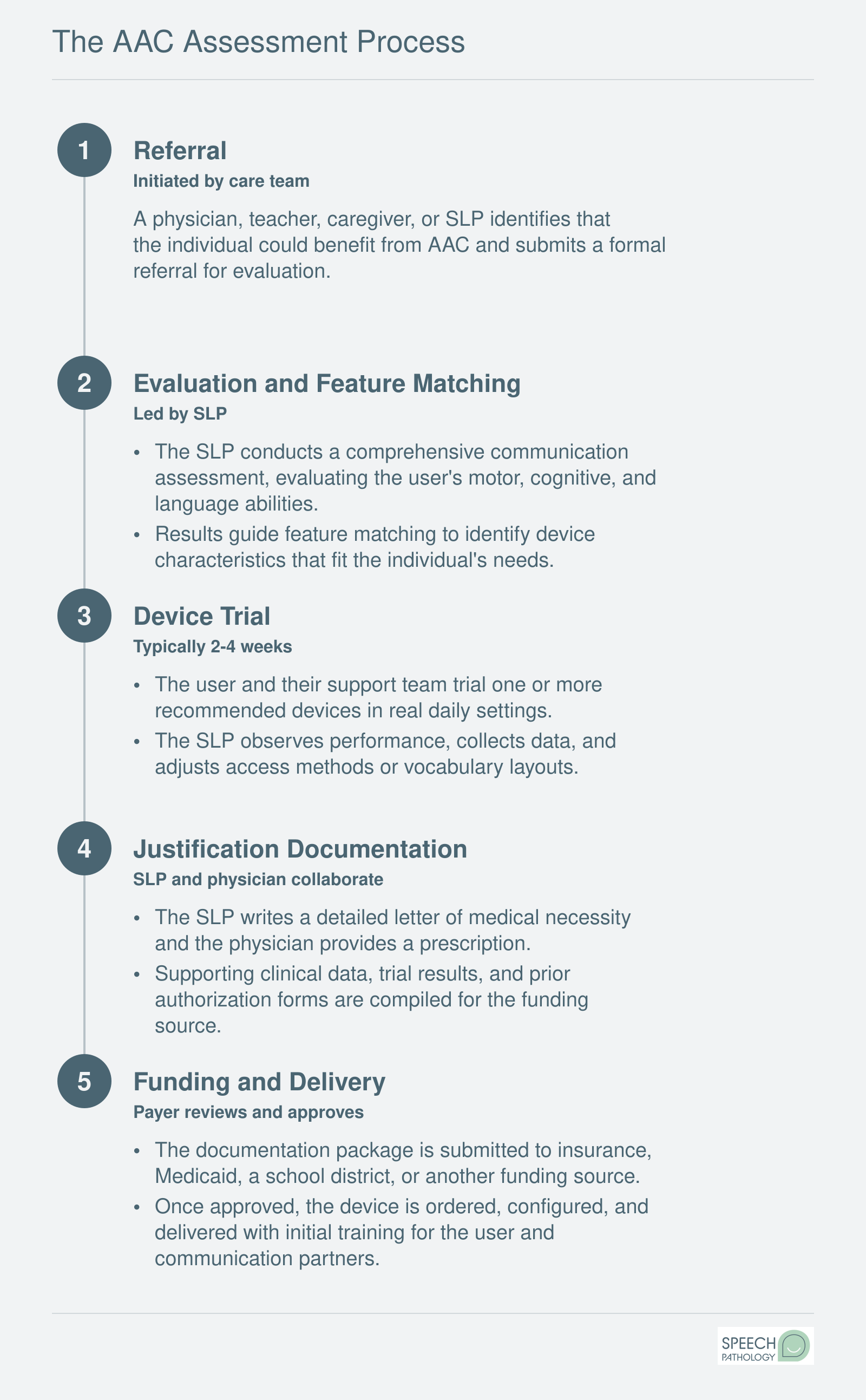
The assessment process typically begins with a referral from a physician, educator, or family member. The SLP then conducts a comprehensive evaluation that includes feature matching, a process of aligning the user's motor, sensory, cognitive, and language abilities with specific device characteristics like access method (touch, switch, eye gaze), vocabulary organization, and symbol type. Clinicians drawing on speech language pathology assessment tools can streamline this phase by pairing standardized measures with AAC-specific protocols.
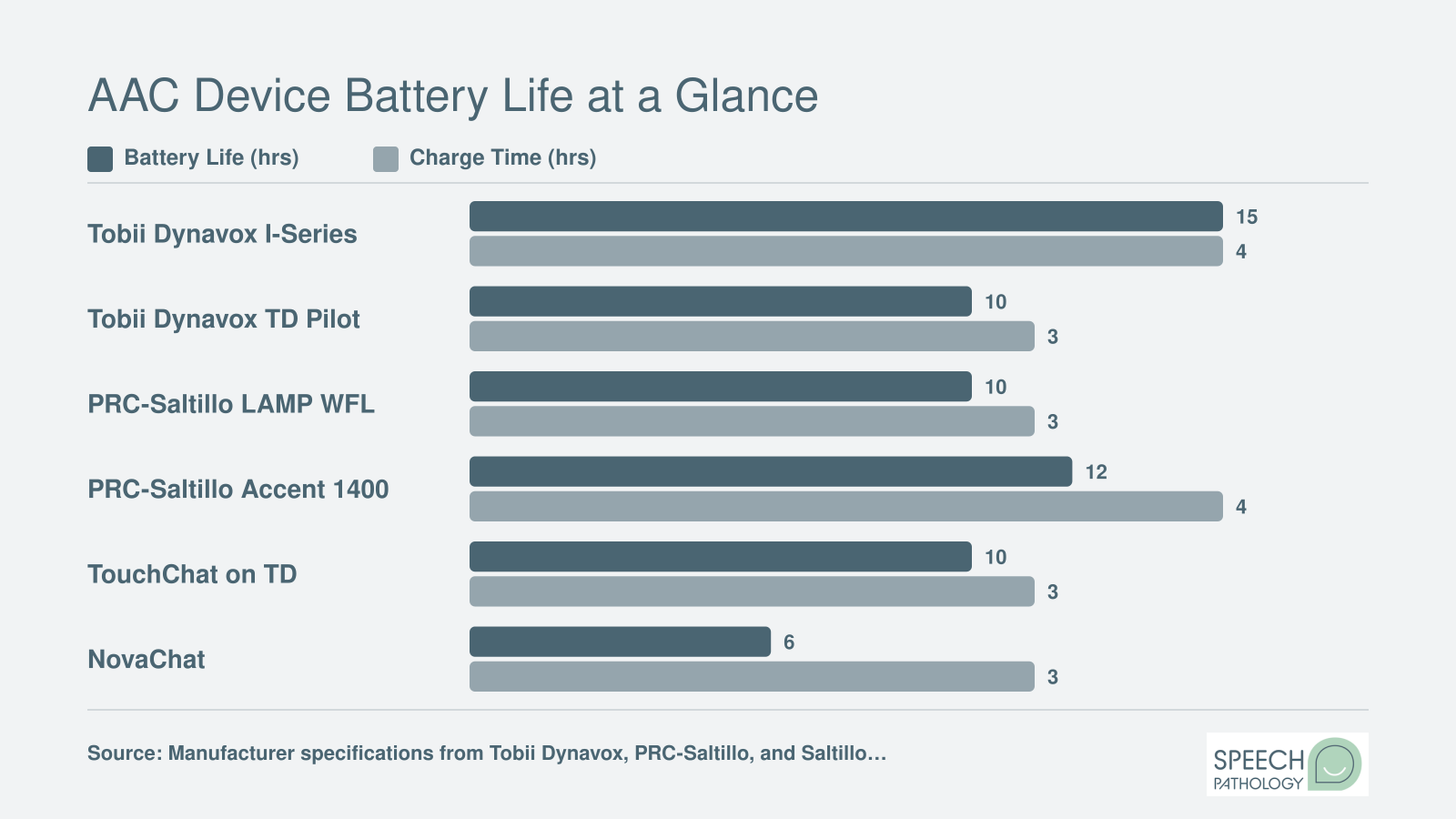
Once the SLP narrows down candidates, a device trial period begins. A 30-day trial is standard practice across the field, and most manufacturers offer loaner devices specifically for this purpose. Medicaid and private insurance carriers generally expect evidence from a trial period before approving funding. During the trial, the SLP collects data on how effectively the user communicates with the device, noting accuracy, speed, engagement, and any barriers that surface in real-world settings.
Interprofessional Collaboration
AAC assessment is rarely a solo effort. Occupational therapists play a critical role in evaluating seating, positioning, and device mounting so the user can access the system comfortably throughout the day. Educators contribute insights about classroom routines and curriculum demands that shape vocabulary selection and device programming. Physical therapists may weigh in on mobility and access, and family members provide essential context about communication needs at home and in the community.
This team-based approach ensures the recommended solution works across all environments, not just the therapy room.
Writing the Justification Letter
After the trial period, the SLP is responsible for writing a detailed justification letter that accompanies any funding request. This document is submitted to insurance companies, Medicaid, or other funding sources and must demonstrate medical necessity. A strong justification letter includes the results of the formal assessment, trial data showing the user's progress with the recommended device, an explanation of why less expensive alternatives are insufficient, and a description of how the device will improve functional communication.
Writing these letters is a skill that SLP graduate programs increasingly emphasize, because a poorly written justification is one of the most common reasons funding requests are denied. Grounding each claim in evidence-based speech therapy techniques strengthens the case and reduces the risk of denial. Clinicians who master this process become invaluable advocates for their clients.
Training and Follow-Up
The assessment does not end when the device is approved and delivered. The SLP provides training to the user, family members, caregivers, and educational staff to ensure consistent use across settings. Follow-up sessions allow the clinician to update vocabulary, adjust settings, and troubleshoot problems. Many SLPs schedule periodic reassessments to confirm the device still meets the user's evolving needs, especially for children whose language skills and physical abilities change rapidly.
For students exploring careers in speech-language pathology, AAC assessment represents one of the most collaborative and technology-forward areas of practice. Pursuing online speech pathology programs can help you build these essential clinical skills through coursework that integrates AAC assessment and assistive technology.