Your Guide to Evidence-Based Practice in Speech-Language Pathology
Learn how to find, evaluate, and apply research evidence to improve clinical outcomes across SLP settings.
By Benjamin Thompson, M.S., CCC‑SLPReviewed by SLP Editoral TeamUpdated August 4, 202625+ min read
Points of interest…
ASHA's three EBP pillars, research evidence, clinical expertise, and client values, guide every sound clinical decision SLPs make.
Roughly 81 percent of SLPs feel confident applying EBP, yet nearly one in five still report uncertainty with the process.
Free databases like ASHA's Evidence Maps and PubMed give clinicians fast access to appraised research for daily practice.
A structured five to seven step EBP cycle works across settings, from pediatric school therapy to adult stroke rehabilitation.
ASHA recognizes more than 60 distinct clinical practice areas within speech-language pathology, yet a typical therapy session lasts just 30 to 60 minutes. Choosing the right approach for a given client, from thousands of published techniques, demands more than intuition. Evidence-based practice is the decision-making framework that bridges that gap: it integrates the best available research evidence, the clinician's own expertise, and the individual client's values and preferences.
EBP is not optional polish on clinical work. It is embedded in ASHA's Code of Ethics, referenced in reimbursement criteria, and increasingly expected by school districts and healthcare systems as a condition of service delivery. For students and professionals navigating the full range of speech pathology careers, understanding EBP is foundational to every clinical decision you will make.
The Three Pillars of EBP: Research Evidence, Clinical Expertise, and Client Values
Evidence-based practice in speech-language pathology rests on three interconnected pillars, as defined in ASHA's position statement (originally published in 2005 and still current as of 2025)1: research evidence, clinical expertise, and client/patient values and circumstances. Understanding how these pillars work together is essential, because EBP is not simply a matter of finding a study and following its protocol. It is a dynamic, ongoing process that requires you to weigh all three elements every time you make a clinical decision.
Research Evidence
Research evidence refers to findings from well-designed studies, systematic reviews, and meta-analyses that inform clinical decision-making. For speech-language pathologists, this might look like consulting a systematic review on LSVT LOUD for individuals with Parkinson's disease before selecting a voice treatment approach. The strength of the evidence matters: a single case study carries different weight than a randomized controlled trial, and clinicians need to evaluate study quality rather than accept results at face value.
Research evidence gives you a starting point, but it is rarely the whole answer. Populations studied in published research may not perfectly match the client sitting across from you, which is exactly why the other two pillars exist.
Clinical Expertise
Clinical expertise is the knowledge, skills, and professional judgment you accumulate through education, supervised practice, and years of hands-on experience. It allows you to adapt research findings to real-world conditions. For example, a clinician working with a patient recovering from a stroke may recognize that afternoon sessions consistently yield lower engagement due to fatigue patterns. Drawing on clinical expertise, the clinician might adjust treatment dosage or scheduling, even if the original research protocol calls for a different frequency, to maximize outcomes for that specific individual. Much of this expertise begins developing during your ASHA clinical fellowship, where supervised caseloads give you the chance to apply research in authentic clinical contexts.
This pillar is what separates thoughtful clinical reasoning from cookbook therapy, where a practitioner follows a rigid set of steps without considering how the intervention fits a particular client.
Client Values and Circumstances
The third pillar centers the client and their family in the decision-making process. A bilingual family, for instance, may prefer that therapy targets be set in their home language rather than English, reflecting cultural priorities and the child's daily communication environment. Client preferences, cultural background, socioeconomic circumstances, and motivation all influence which interventions are appropriate and sustainable.
Ignoring this pillar risks recommending treatments that a client cannot access, does not want, or will not follow through on outside of the therapy room.
What About the "Fourth Pillar"?
If you have encountered references to four key components of EBP, you are not imagining things. Some frameworks add a fourth element, often described as clinical context or practice setting, which accounts for factors like available resources, caseload size, and organizational policies. ASHA's model, however, treats these contextual factors as part of clinical expertise and client circumstances rather than as a standalone pillar.1 The distinction is largely one of framing, not a fundamental disagreement. If your coursework or workplace uses a four-part model, the core principle remains the same: integrate multiple sources of information rather than relying on any single one.
EBP as a Living Process
ASHA frames evidence-based practice as a dynamic process, not a one-time literature search you perform at the start of a case and never revisit. New research emerges, client needs evolve, and your own expertise grows over time. The ASHA Practice Portal is continuously updated to reflect current evidence across communication disorders, and events like the 2024 Research Roundtables provide clinicians with opportunities to engage with the latest findings.
For students and early-career SLPs, the key takeaway is this: mastering EBP means learning to hold all three pillars in balance. Research keeps your practice grounded in science. Clinical expertise lets you tailor that science to the person in front of you. And centering client values ensures that the care you provide is not only effective but meaningful to the people who receive it.
Why Evidence-Based Practice Matters for SLPs
Evidence-based practice is not simply an academic ideal. It shapes the quality of care that clients receive, the professional standing of clinicians, and the way speech-language pathology services are funded and evaluated. Understanding why EBP matters can motivate you to make it a consistent part of your clinical routine rather than an occasional exercise.
Better Outcomes Through Informed Decision-Making
When clinicians select interventions backed by current research, therapy tends to be more efficient and more effective. While large-scale outcome studies specific to speech-language pathology are still emerging, the broader healthcare literature consistently shows that EBP-guided care reduces variability in treatment quality and improves patient satisfaction. Research from George Washington University examining SLP perspectives on EBP found that clinical supervision is a key facilitator of evidence-based practice, suggesting that mentorship environments help translate research knowledge into measurable gains for clients.1 The takeaway for students and early-career SLPs is clear: building EBP skills now sets the stage for stronger clinical results throughout your career.
An Ethical Responsibility
ASHA's Code of Ethics, specifically Principle I, requires speech-language pathologists to provide services competently and to stay current with developments in the profession. In practice, this means relying on outdated or unsupported techniques when better-supported alternatives exist is not just inefficient; it raises genuine ethical concerns. Clinicians working within the SLP scope of practice already navigate a broad range of responsibilities, and committing to EBP is one of the most direct ways to honor your obligation to each client you serve.
Meeting Payer and School-District Expectations
Third-party payers, including private insurance companies and Medicaid programs, increasingly require documentation that chosen interventions have an evidence base. In school settings, IEP teams may ask clinicians to justify the approaches they recommend. Being able to cite relevant research strengthens your clinical rationale, supports reimbursement claims, and builds trust with families and interdisciplinary colleagues. SLPs who struggle to articulate the evidence behind their methods may find it harder to secure approval for the services their clients need.
The Accreditation Pipeline
The expectation that SLPs will practice in an evidence-based manner begins well before the first day on the job. The Council on Academic Accreditation in Audiology and Speech-Language Pathology (CAA) requires accredited graduate programs to integrate EBP into their curricula. Students learn to formulate clinical questions, search the literature, and appraise research quality as core competencies. This academic foundation creates a professional pipeline: by the time you earn your Certificate of Clinical Competence, you are expected to carry those skills into every clinical decision you make.
Recent survey data highlights that accessibility of research remains a notable barrier to consistent EBP adoption among practicing SLPs.1 Recognizing that challenge early, and learning how to navigate research databases efficiently, gives you an advantage as you transition from student to clinician. The sections ahead will walk you through exactly how to do that.
According to a 2022 survey, roughly 81 percent of speech-language pathologists reported feeling confident in their ability to apply evidence-based practice principles. While that number sounds encouraging, it also means nearly one in five SLPs still feel uncertain, highlighting a continued need for accessible EBP training and mentorship across the profession.
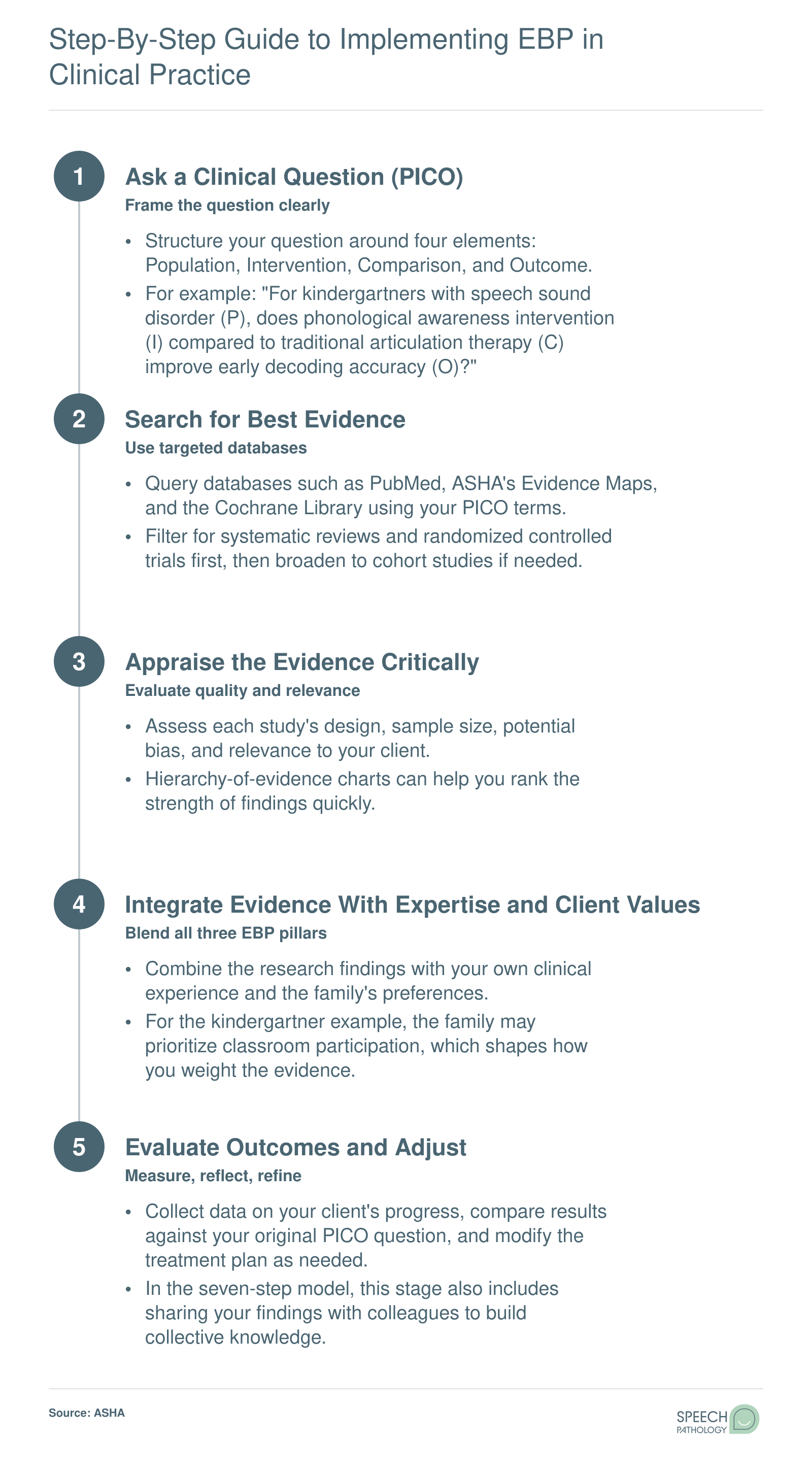
Step-By-Step Guide to Implementing EBP in Clinical Practice
Most clinicians learn a core five-step EBP cycle, but you may also encounter a seven-step version. The expanded model simply adds "cultivate a spirit of inquiry" before Step 1 and "disseminate results" after Step 5. Both frameworks follow the same logic. Here is the five-step cycle in action, illustrated by a school-based SLP asking whether phonological awareness intervention improves decoding skills for a kindergartner with a speech sound disorder.
How to Search and Appraise SLP Research: A Practical Walkthrough
Finding and evaluating research does not have to feel overwhelming, even for clinicians juggling packed caseloads. The process becomes far more manageable when you break it into two clear phases: asking the right question, then reading the evidence with a critical eye.
Start With a PICO Question
A well-formed clinical question keeps your search focused. The PICO framework organizes your question around four elements:
Population: Who is the client or client group? (e.g., adults post-stroke with non-fluent aphasia)
Intervention: What treatment are you considering? (e.g., constraint-induced language therapy)
Comparison: What alternative would you otherwise use? (e.g., traditional naming drills)
Outcome: What change do you hope to see? (e.g., improvement in functional, everyday communication)
Putting this together, your searchable question might read: "For adults with non-fluent aphasia following stroke, does constraint-induced language therapy lead to greater improvement in functional communication compared to traditional naming drills?" With that sentence in hand, you can pull out key search terms and head into a database with purpose instead of scrolling aimlessly.
Understand the Evidence Hierarchy
Not all studies carry equal weight. In most health professions, the evidence hierarchy looks like this, from strongest to weakest:
Systematic reviews and meta-analyses
Randomized controlled trials (RCTs)
Cohort and case-control studies
Case series and case reports
Expert opinion and consensus statements
In communication sciences, however, single-subject experimental designs deserve special attention. Because many speech-language pathology populations are small or highly heterogeneous, well-controlled single-subject studies with replicated effects can provide strong evidence for individual treatment decisions. ASHA recognizes these designs as a legitimate and valuable level of evidence, so do not dismiss a study simply because it reports on one or a handful of participants. Understanding these nuances is part of the broader speech language pathologist education requirements that prepare clinicians for real-world practice.
Three Quick Appraisal Questions for Busy Clinicians
When time is short, you can gauge a study's relevance by asking just three questions:
Was the sample comparable to my client? Consider age, diagnosis severity, time post-onset, and cultural or linguistic background. A study of young adults with mild word-finding difficulty may not generalize well to an older adult with severe global aphasia.
Was the outcome measure functionally relevant? Gains on a standardized naming test matter, but improvements in real-world conversational participation often matter more to clients and families.
Was the effect size clinically meaningful? Statistical significance tells you whether a finding is likely real; effect size tells you whether the difference is large enough to matter in daily life. A statistically significant gain of one point on a 60-point scale may not change how a client communicates at home.
Running every article through these three filters takes only a few minutes and helps you decide whether to apply, adapt, or set aside a study's findings.
When the Evidence Is Thin
Sometimes your PICO search turns up very little, especially for newer or less-studied interventions. It is important to remember that an absence of evidence is not the same as evidence that something does not work. Emerging approaches may simply lack the research base yet. If your clinical expertise suggests a treatment has promise and your client's values and preferences support giving it a try, a carefully monitored trial can be entirely appropriate. Document your rationale, track outcomes, and revisit the literature as new studies appear. That combination of professional judgment and ongoing data collection is itself the heart of evidence-based practice.
Best EBP Databases and Resources for Speech-Language Pathologists
Knowing where to find high-quality research is half the battle when you are putting evidence-based practice into action. The good news: several databases are built specifically for speech-language pathologists, and many of them are completely free.1 Below is a practical comparison of the tools clinicians and students rely on most, with notes on cost, scope, and the best scenario for each.
Free, SLP-Focused Databases
ASHA Evidence Maps: Curated by the American Speech-Language-Hearing Association, these maps organize systematic reviews and evidence summaries across core SLP topics such as aphasia, dysphagia, childhood apraxia of speech, and augmentative and alternative communication.2 The maps rate the strength of available evidence, making them a logical first stop when you need a quick overview. Access is open to everyone, no ASHA membership required.
speechBITE: This database catalogs over 5,000 intervention studies spanning articulation, fluency, voice, and swallowing disorders. Each study receives a quality rating, and filters let you narrow results by population, design, or disorder. It is free with optional newsletter signup. The main limitation is that it focuses on intervention research, so diagnostic or assessment studies may require a separate search.
Broad Biomedical and Review Databases
PubMed: Operated by the National Library of Medicine, PubMed offers the widest net for biomedical literature, including strong coverage of language disorders, neurogenic communication, and pediatric speech research.4 Abstracts are always free, and many full-text articles are available through PubMed Central. Some journals, however, sit behind paywalls, which can be a hurdle for clinicians without institutional library access.
Cochrane Library: When you need the gold standard in systematic reviews, Cochrane is the place to look. It houses rigorously conducted reviews on topics such as speech therapy for autism, post-stroke aphasia rehabilitation, and stuttering interventions.5 Review summaries are free and written in plain language, though access to certain trial records may require a subscription or institutional login.
TRIP Database: TRIP aggregates content from over 70 sources, pulling in clinical guidelines, synopses, and evidence-based textbooks alongside primary research.6 The free basic version is useful for quick searches on topics like dysphagia management or pediatric language delay. A Pro subscription (roughly $50 per year) unlocks advanced features including a PICO-structured search tool, which is worth considering if you conduct clinical questions regularly.
Curated Summaries for Busy Clinicians
The Informed SLP: This subscription service reviews over 100 journals each month and distills findings into plain-language summaries paired with implementation guides.7 At approximately $10 per month, it also offers continuing education credits. It is not a primary research database, so you would still turn to PubMed or speechBITE for an exhaustive literature search. However, for clinicians in school settings or private practice who have limited time, it bridges the gap between published research and everyday clinical decisions.
A Note on Access for Clinicians Outside Universities
If you work in a school district, speech language pathology career outlook, or healthcare facility without a university library portal, prioritize the free tools first. ASHA Evidence Maps, speechBITE, and PubMed abstracts together cover a wide range of clinical questions at no cost. For full-text articles locked behind paywalls, interlibrary loan services, open-access repositories, and author preprints can fill many gaps. The TRIP Database's free tier and The Informed SLP's affordable subscription round out a practical toolkit that does not depend on institutional access.
Building a short list of two or three go-to databases, rather than searching everywhere at once, helps you develop efficient habits. Start with ASHA Evidence Maps for a topic overview, move to speechBITE or PubMed for specific intervention studies, and consult Cochrane when a systematic review exists. Over time, this layered approach becomes second nature and keeps evidence-based decision-making manageable even on a busy caseload.
Questions to Ask Yourself
When was the last time you changed a therapy approach based on new research rather than habit?
Sticking with familiar techniques can feel efficient, but research in communication sciences evolves quickly. Regularly revisiting your methods against current findings helps ensure clients receive the most effective interventions available.
Do you have a go-to database you search before starting with a new client, or do you rely solely on what you learned in graduate school?
Graduate training provides a strong foundation, yet best practices shift as new studies are published. Building a habit of checking databases like PubMed or the ASHA Evidence Maps before planning treatment keeps your clinical decisions grounded in the latest evidence.
How often do you formally ask clients or families what outcomes matter most to them?
Client and family priorities are one of the three core pillars of evidence-based practice. Without structured conversations about goals and values, even a well-researched treatment plan may miss what matters most to the people you serve.
EBP in Action: Pediatric Vs. Adult Applications
Evidence-based practice looks different depending on whether you are working with a three-year-old in a school therapy room or a 68-year-old recovering from a stroke in a skilled nursing facility. The table below compares how the three pillars of EBP play out across pediatric and adult speech-language pathology settings, highlighting how clinicians adapt their decision-making process to each population.
Dimension
Pediatric SLP
Adult SLP
Typical Clinical Questions
Which intervention approach best addresses childhood apraxia of speech (CAS)? For example, should a clinician choose PROMPT (Prompts for Restructuring Oral Muscular Phonetic Targets) or a traditional articulation approach? ASHA's Practice Portal rates PROMPT as having emerging evidence for CAS, so the clinician must weigh limited research alongside hands-on clinical judgment.
What treatment intensity produces the best functional outcomes for post-stroke aphasia? Clinicians often turn to large systematic reviews, such as the Brady et al. Cochrane review on speech and language therapy for aphasia, to compare dosage schedules and therapy types supported by stronger bodies of research.
Evidence Availability
Generally thinner, especially for low-incidence conditions like CAS or pediatric fluency disorders in multilingual children. Randomized controlled trials are harder to conduct with young populations, so clinicians frequently rely on smaller case series or single-subject designs. This means clinical expertise and family input carry relatively more weight in decision-making.
Broader and more robust for high-prevalence conditions such as aphasia, dysarthria, and dysphagia. Multiple Cochrane reviews and large-scale RCTs exist, giving clinicians a stronger research foundation. Gaps remain for less common adult conditions and for culturally diverse populations.
Role of Caregiver or Client Values
Parents and caregivers are central to goal-setting and carry-over activities. A family's daily routines, cultural priorities, and comfort with home practice heavily influence which therapy approach is realistic and sustainable. For a child with CAS, a caregiver who can support frequent, short practice sessions at home may tip the decision toward a motor-learning approach.
The patient's own recovery priorities guide treatment planning. An adult with aphasia may prioritize returning to work conversations over written communication, shaping the clinician's choice of therapy targets. Spouses and adult children also contribute, but the client's autonomy is the primary driver.
Common Outcome Measures
Standardized articulation and language tests (e.g., Goldman-Fristoe Test of Articulation, CELF), percent consonants correct, intelligibility ratings, and curriculum-based measures tied to educational benchmarks. Progress is often tracked across an academic year.
Functional communication scales (e.g., ASHA NOMS, Western Aphasia Battery, FOIS for dysphagia), patient-reported outcome measures, and quality-of-life inventories. Progress is often measured in shorter rehabilitation windows aligned with insurance or facility discharge timelines.
Setting Constraints
School-based SLPs must align therapy with Individualized Education Program (IEP) goals and work within group scheduling, limited session frequency, and academic calendars. These constraints can make it difficult to implement high-dosage protocols that research may recommend.
Hospital and skilled nursing facility SLPs operate under medical-model timelines, insurance authorization limits, and interdisciplinary team schedules. High-intensity treatment may be feasible in acute rehab but harder to sustain after discharge, requiring creative planning for outpatient or teletherapy continuation.
Common Barriers to EBP and How to Overcome Them
Knowing the principles of evidence-based practice is one thing. Consistently applying them in a busy clinical schedule is another. Research on EBP adoption in speech-language pathology has repeatedly identified a handful of obstacles that trip up both new graduates and seasoned clinicians. The good news is that each barrier has a practical workaround, and the skill of implementing EBP genuinely improves with repetition.
Lack of Time
Time is the barrier SLPs cite most often. Between documentation, direct treatment sessions, and meetings, carving out hours for literature searches can feel impossible. A high-impact shortcut is to rely on pre-appraised resources rather than conducting raw database searches from scratch. ASHA's Evidence Maps, for example, organize and summarize research by clinical topic, so you can locate relevant findings in minutes instead of hours. Systematic reviews and clinical practice guidelines also compress hundreds of studies into one readable document, saving enormous amounts of reading time.
Limited Access to Research
Not every workplace provides subscriptions to major journals. If paywalls are blocking your progress, remember that many databases offer free content. PubMed Central archives thousands of open-access articles, and Google Scholar often surfaces freely available manuscript versions. Interlibrary loan services through local or university libraries can fill in the gaps. ASHA members also gain access to journal content through their membership, which is worth exploring if you have not already.
Difficulty Appraising Study Quality
Reading a research article is not the same as evaluating whether its conclusions are trustworthy. If critical appraisal feels daunting, start with a structured checklist. Tools like the CASP (Critical Appraisal Skills Programme) checklists walk you through questions about study design, bias, and applicability in a step-by-step format. Joining or forming a journal club, whether at your workplace or through an online community, makes this process collaborative and far less intimidating.
Workplace Culture That Does Not Prioritize EBP
Some clinical settings default to "the way we've always done it." Shifting that culture starts with small, visible wins. Choose one client or one intervention area, apply an evidence-based approach, and track outcomes. Presenting concrete data to supervisors, such as improved scores or faster progress toward goals, builds a compelling case that EBP is worth the investment.
Building Momentum Over Time
New clinicians sometimes feel pressure to overhaul every aspect of their practice at once. That expectation is unrealistic and counterproductive. A more sustainable approach is to start with one well-formed clinical question per month. Investigate it, apply what you find, and reflect on the result. Over a year, that adds up to twelve evidence-informed decisions that gradually reshape your practice.
Mentorship and peer collaboration lower the barrier to entry significantly. ASHA Special Interest Groups (SIGs) connect you with clinicians who share your focus area, and SLP-focused social media communities regularly discuss current research in accessible terms. Whether you are completing your ASHA CF requirements or well into your career, the path to consistent evidence-based practice is not about perfection on day one. It is about steady, informed improvement over the course of a career.
Integrating EBP With Teletherapy and Emerging Service Models
The rapid expansion of telepractice in speech-language pathology, especially since 2020, has raised an important question for clinicians committed to evidence-based practice: do interventions validated in face-to-face settings hold up when delivered through a screen? The short answer is encouraging but incomplete. ASHA recognizes telepractice as an appropriate service delivery model, and a growing body of post-2020 research indicates that many SLP interventions produce comparable outcomes whether delivered remotely or in person. Still, EBP demands that clinicians look closely at the evidence rather than assume blanket equivalence. If you are considering building a remote caseload, our guide on how to start a telepractice SLP walks through the logistics and licensure steps.
Where the Evidence Is Strong
Several areas of SLP practice have accumulated solid support for teletherapy delivery. Language intervention for school-age children, fluency treatment programs, and voice therapy protocols have each shown promising results in remote formats. Parent-coached early language interventions have also translated well, partly because the coaching model naturally fits a virtual platform where the caregiver is the hands-on partner. For students exploring slp career paths, these are areas where you can feel confident that EBP and telepractice align.
Where Evidence Gaps Remain
Not every clinical scenario has the same level of support. Key gaps include:
Assessment reliability: Standardized testing administered via telehealth may introduce variability related to audio quality, internet lag, or limited ability to observe subtle motor behaviors.
Very young children and severe cognitive impairment: Maintaining engagement and ensuring valid data collection remotely is more difficult with these populations, and the research base is still thin.
Tactile-dependent interventions: Approaches like PROMPT therapy, which rely on physical touch cues to guide articulatory movement, cannot be replicated through a screen. Clinicians must either identify alternative techniques with their own evidence base or combine telepractice with periodic in-person sessions.
Building Practice-Based Evidence in Real Time
When you adapt an evidence-based intervention for remote delivery, treat the adaptation itself as a data opportunity. Document exactly what you changed (session length, materials, cueing strategies, caregiver involvement) and track client outcomes systematically. This kind of practice-based evidence helps fill the gaps the published literature has not yet addressed and strengthens your clinical decision-making over time. Even simple pre- and post-treatment measures can reveal whether the modified approach is working for a given client.
Other Emerging Models Worth Evaluating
Telepractice is not the only service model reshaping SLP practice. Interprofessional collaborative practice, where SLPs work alongside educators, occupational therapists, and psychologists, is gaining traction in both medical and school settings. Coaching-based service delivery shifts the clinician's role from direct interventionist to a guide who empowers caregivers or teachers. Classroom-embedded therapy integrates speech and language goals into the natural academic environment rather than pulling students out for isolated sessions.
Each of these models has intuitive appeal, but intuition is not evidence. As a current or future SLP, your responsibility is to evaluate the research supporting each model for the specific population and goals you are addressing. ASHA's Practice Portal and similar databases can help you locate relevant systematic reviews and clinical guidelines so you are making informed, evidence-driven choices rather than following trends.
Frequently Asked Questions About EBP in Speech-Language Pathology
Evidence-based practice raises many questions for students and working clinicians alike. Below are answers to the most common questions about EBP in speech-language pathology, drawn from ASHA guidelines and current clinical literature.
What are evidence-based practices in SLP?
Evidence-based practices in SLP are clinical approaches that integrate the best available research evidence with a clinician's professional expertise and the individual preferences, values, and needs of the client. Rather than relying on tradition or intuition alone, SLPs use a structured process to find, evaluate, and apply research findings to assessment and treatment decisions across all areas of communication and swallowing disorders.
What are the 4 key components of evidence-based practice?
The four key components are: (1) formulating a clear clinical question, (2) searching for the best available research evidence, (3) critically appraising that evidence for quality and relevance, and (4) integrating the appraised evidence with clinical expertise and client values to make a treatment decision. Some frameworks add a fifth component: evaluating the outcome of the decision.
What are the 7 steps of evidence-based practice?
The seven steps typically include: (1) cultivate a spirit of inquiry, (2) formulate a focused clinical question using a framework such as PICO, (3) search for the best evidence, (4) critically appraise the evidence, (5) integrate evidence with clinical expertise and client preferences, (6) evaluate the outcome of the practice change, and (7) disseminate results to colleagues or through professional channels.
Why is evidence-based practice important in speech pathology?
EBP is important because it helps SLPs deliver the most effective, ethical, and accountable care possible. It reduces reliance on outdated methods, improves client outcomes, supports reimbursement justifications, and aligns practice with ASHA's Code of Ethics. For students and new graduates, building EBP skills early strengthens clinical reasoning and prepares them for the evolving demands of the profession.
How do you integrate EBP into daily SLP clinical practice?
Start by building clinical questions around the clients you see each day. Set aside short blocks of time to search trusted databases, read systematic reviews, and discuss findings with colleagues. Use outcome measures to track whether a chosen intervention is working. Over time, these habits become routine. Journal clubs, mentorship, and resources on speechpathology.org can also support consistent EBP integration.
What are the best EBP databases for speech-language pathologists?
Key databases include PubMed, the Cochrane Library, ASHA's Evidence Maps, and speechBITE (Speech Pathology Database for Best Interventions and Treatment Efficacy). CINAHL and PsycINFO are also valuable for communication sciences research. Many university libraries provide free access to these tools, and ASHA members can use the Practice Portal for curated systematic reviews on specific clinical topics.
Does evidence-based practice mean I can only use randomized controlled trials?
No. While randomized controlled trials are considered a high level of evidence, EBP values the best available evidence, which may include single-subject designs, cohort studies, case series, or expert consensus when stronger designs do not yet exist. The key is to critically appraise whatever evidence is available and combine it with clinical expertise and client input rather than waiting for a perfect study.
How can new graduate SLPs start building EBP habits?
New graduates can begin by practicing PICO question formulation during their clinical fellowship. Joining or starting a journal club, bookmarking reliable databases, and following ASHA's Evidence Maps are low-effort, high-impact starting points. Seeking mentors who model EBP, attending continuing education on research appraisal, and exploring resources on speechpathology.org will help turn these habits into a sustainable part of everyday practice.
Evidence-based practice is not an abstract ideal you leave behind in graduate school. It is a daily clinical habit, built on the same cycle you have seen throughout this guide: ask a focused question, find the best available research, and weigh that evidence alongside your clinical expertise and your client's priorities.
Here is one concrete step you can take this week. Choose a single client on your caseload, form a PICO question about their treatment, and search one of the databases listed earlier in this article. That is all it takes to start. Even small, consistent EBP habits compound over the course of a career, leading to measurably better outcomes for the people who depend on your skills.