Dysarthria Symptoms and How It's Diagnosed
Dysarthria can look and sound different from one person to the next, but several hallmark symptoms overlap across types. Recognizing these signs is the first step; confirming the diagnosis and pinpointing the type requires a structured evaluation by a speech-language pathologist (SLP), often working alongside a neurologist.
Hallmark Symptoms to Watch For
Because dysarthria affects the muscles used for speech, its symptoms center on how speech sounds and how well a listener can understand it. Common signs include:
- Slurred or slow speech: Words may run together or be produced at an unusually slow rate, making conversation effortful.
- Abnormal pitch or rhythm: Speech may sound monotone, unusually high or low, or have an irregular, "scanning" quality where syllables are evenly stressed.
- Nasal or breathy voice quality: Air may escape through the nose during speech (hypernasality), or the voice may sound weak and breathy due to poor vocal fold closure.
- Difficulty controlling loudness: Volume may be too soft for listeners to hear comfortably or may fluctuate unpredictably.
- Drooling and swallowing difficulty: Reduced oral motor control can lead to difficulty managing saliva, and swallowing problems (dysphagia) frequently co-occur.
- Reduced intelligibility: The cumulative effect of these features is that listeners struggle to understand the speaker, especially in noisy environments or over the phone.
Symptoms may appear suddenly after a stroke or traumatic brain injury, or they may develop gradually alongside a progressive neurological condition like Parkinson's disease or ALS.
The SLP Diagnostic Process
A comprehensive dysarthria evaluation blends clinical observation with standardized tools. SLPs typically use three layers of assessment, drawing on SLP assessment tools designed for motor speech disorders.
Perceptual analysis forms the foundation. The clinician listens carefully to connected speech, noting deviations in articulation, resonance, phonation, respiration, and prosody. Diadochokinetic tasks, which ask the patient to rapidly repeat syllable sequences like "puh-tuh-kuh," help reveal breakdowns in motor speed and coordination.
Instrumental measures add objective data. Nasometry quantifies nasal airflow during speech, acoustic analysis software tracks pitch, loudness, and voice quality over time, and videofluoroscopy can visualize velopharyngeal function during speech and swallowing.
Intelligibility testing rounds out the picture. The SLP may use sentence or single-word identification tasks in which a listener (unfamiliar with the speaker) scores how many words they can correctly identify. This provides a functional measure of how well the person communicates in real-world conditions.
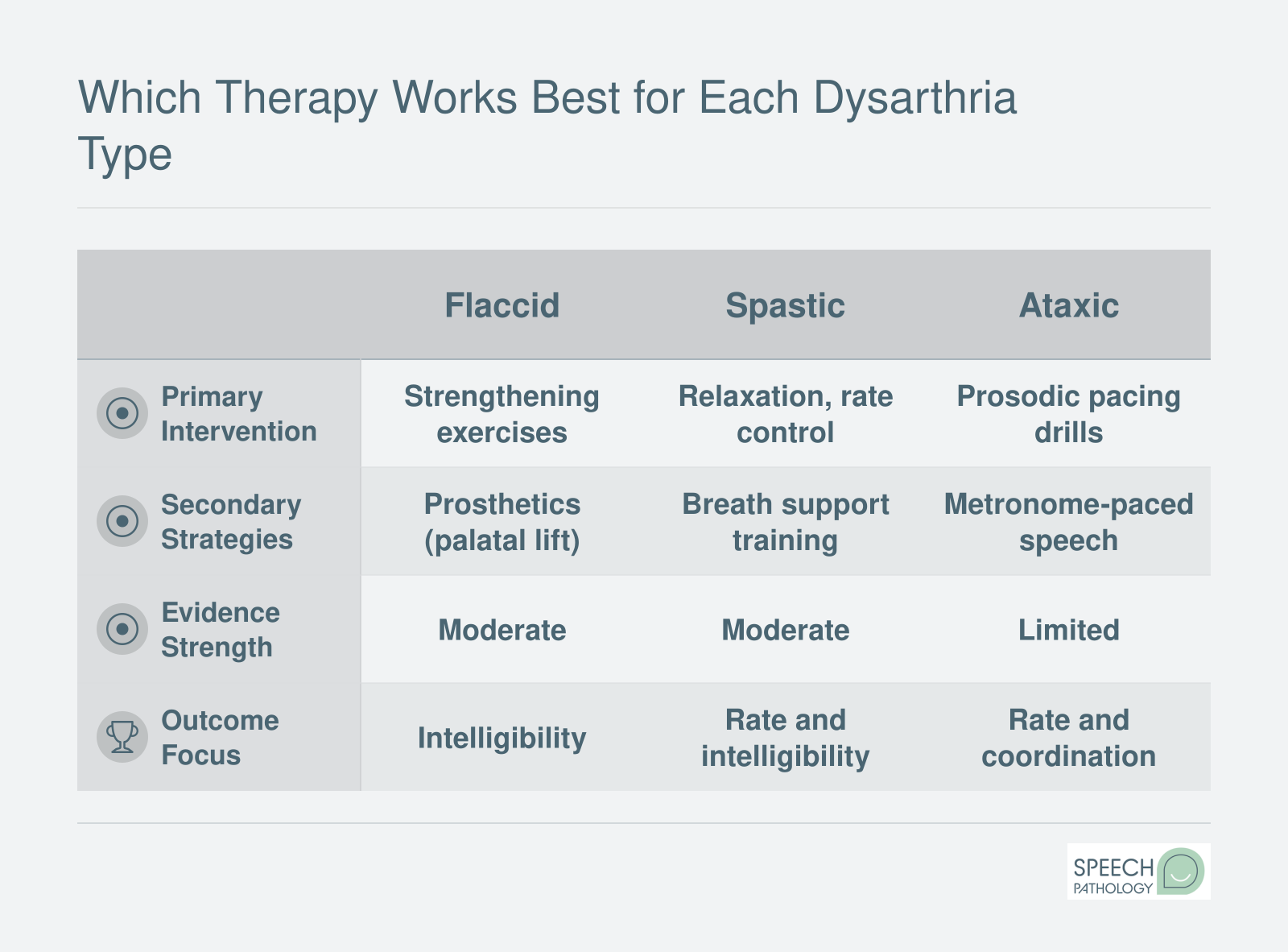
Classifying Dysarthria Type
Most clinicians rely on the Mayo Clinic classification system developed by Darley, Aronson, and Brown. This framework, still considered the standard in the field, categorizes dysarthria into types based on clusters of perceptual speech features. For example, a pattern of imprecise consonants, slow rate, and excess and equal stress points toward ataxic dysarthria, while a strained, strangled voice quality with short phrases suggests spastic involvement. Matching the perceptual profile to a type helps the SLP predict which neurological systems are involved and guides treatment planning.
Collaborating With Neurology
Diagnosis does not stop at the speech level. Identifying the underlying neurological cause is essential for prognosis and treatment. SLPs frequently collaborate with neurologists who use brain imaging (MRI, CT), nerve conduction studies, or blood work to pinpoint the site and nature of the lesion. In cases where the cause is unknown at referral, the specific dysarthria type identified by the SLP can actually help narrow the neurological differential, making the SLP evaluation a valuable piece of the diagnostic puzzle. For severe cases where natural speech becomes unreliable, the evaluation may also explore AAC devices to support functional communication.