How Speech Therapy Helped One Autistic Child Find Her Voice
A parent's real story of AAC, apraxia, and years of speech therapy progress — plus what SLPs and families can learn from the journey.
By Benjamin Thompson, M.S., CCC‑SLPReviewed by SLP Editoral TeamUpdated July 10, 202625+ min read
Points of interest…
Annie spoke her first words after age 10 following years of speech therapy and AAC use.
PECS and ProLoQuo2Go support language development rather than replacing spoken communication.
Family-centered, multimodal therapy redefines communication success well beyond speech alone.
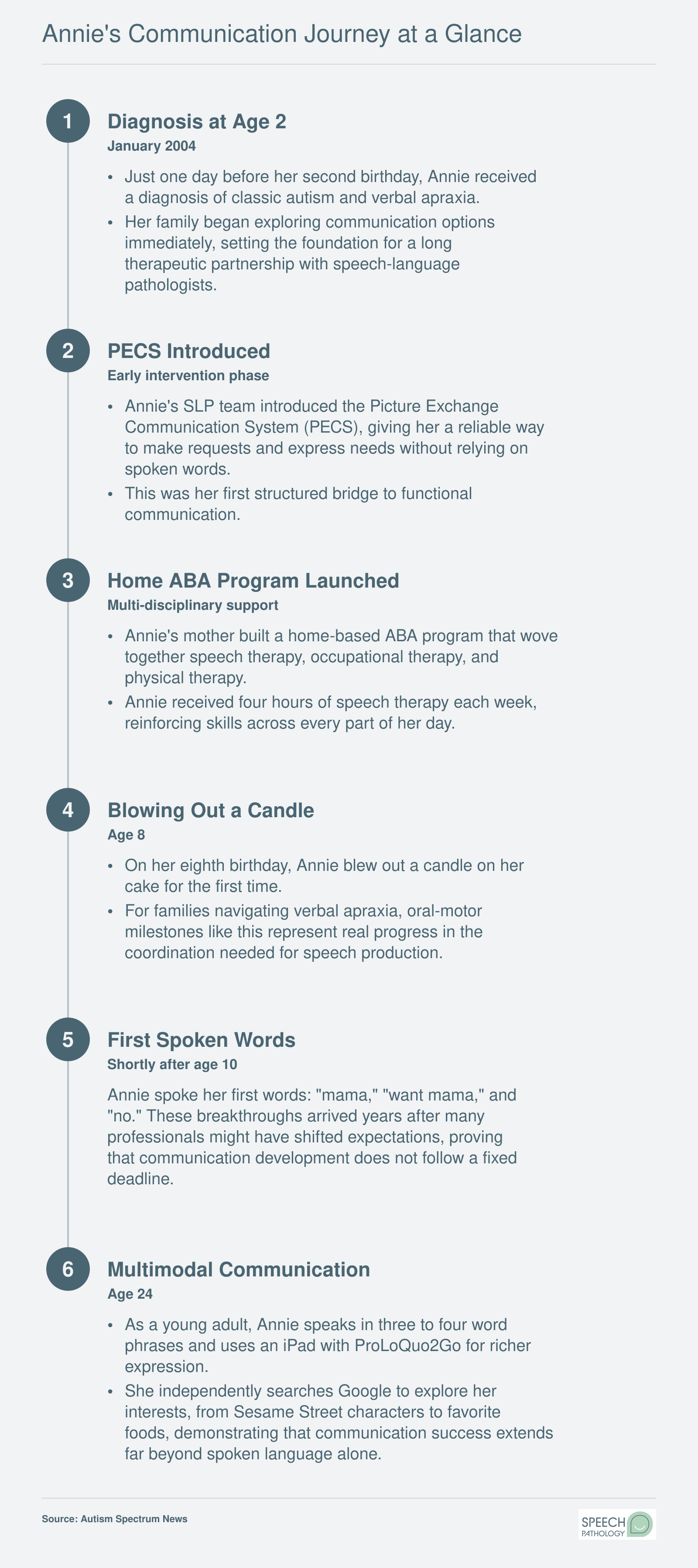
On January 8, 2004, the day before her second birthday, a girl named Annie received a diagnosis of classic autism and verbal apraxia. She would not speak her first words for another eight years. Annie's mother spent those years building a home therapy program, coordinating four hours of weekly speech services, and learning to read communication in forms she had never anticipated.
Annie began with PECS boards as a toddler, moved to the ProLoQuo2Go app on an iPad, and spoke "mama" shortly after turning ten. At 24, she uses three to four word phrases alongside her device. Her story, shared through one mom's journey with autism communication, is a two-decade case study in what speech-language pathologists and families gain when they measure progress by functional communication rather than spoken language alone.
Annie's Story: From Diagnosis to First Words
In pediatric speech-language pathology, the shift toward multimodal communication has reframed what success looks like for children with autism: celebrating any form of functional communication, not just spoken words. Annie's journey, as shared by her mother with Autism Spectrum News, exemplifies this evolution.1
A Life-Changing Diagnosis
On January 8, 2004, one day before Annie's second birthday, she was diagnosed with classic autism and verbal apraxia.1 The dual diagnosis explained her minimal speech and limited social engagement. Her therapy team immediately introduced the Picture Exchange Communication System (PECS), teaching Annie to exchange picture cards for wants and needs. Early intervention was intensive: four hours of speech therapy per week alongside enrollment at Devereux Center for Autism Research and Education Services (CARES). For Annie's mother, the diagnosis was devastating but also clarifying, setting the stage for a years-long commitment to therapy at home and in clinical settings.
Building a Comprehensive Home Program
Annie's mother crafted a home-based program rooted in applied behavior analysis (ABA) that integrated speech, occupational, and physical therapy.1 Speech-language pathologists working with autism coached the family on PECS implementation, oral motor exercises, and consistent modeling. The multidisciplinary approach aimed to build foundational communication skills while addressing sensory and motor challenges. Four hours of dedicated speech therapy each week became the cornerstone of this routine, supplemented by the structured environment at CARES. The mother became a partner in therapy, learning to weave communication attempts into everyday moments.
The Emotional Turning Point
Around Annie's fifth birthday, her mother mourned the possibility that Annie might never speak.1 Many families experience this moment of reckoning, and for SLPs, it is a critical time to guide caregivers toward acceptance of alternative communication methods. A significant milestone came three years later: on her eighth birthday, Annie blew out the candle on her cake. This oral motor achievement, directly tied to speech therapy, signaled emerging control and gave renewed hope. It was a small act that carried deep emotional weight, proof that progress was happening.
A Breakthrough After Years of Therapy
Shortly after turning 10, Annie spoke her first words: "mama," "want mama," and "no."1 Her mother described the moment as transformative. Today, at 24, Annie uses 3-4 word phrases verbally and relies on an iPad with ProLoQuo2Go for fuller expression. Her story is not one of rapid progress but of steady, supported gains over decades, demonstrating that communication breakthroughs can happen well beyond early childhood. Annie's experience sets the stage for the clinical insights that follow, illustrating how persistence, multimodal tools, and family partnership shape outcomes.
What Speech Therapy Looks Like for Children With Autism
Speech therapy for an autistic child is not one fixed routine. It is a set of carefully chosen activities, tools, and interaction strategies that shift depending on the child's age, communication profile, and individual needs. If you have ever wondered what actually happens during a session, here is a concrete picture drawn from the approaches that carry the strongest current evidence.
How Sessions Differ by Age and Setting
For a toddler who has just received an autism diagnosis, speech therapy often takes place on the floor. The autism speech therapy process at this stage has the speech-language pathologist following the child's lead during play, modeling language around whatever toy or object catches the child's attention. Sessions typically last 30 to 45 minutes once or twice a week, and they may happen in a clinic playroom, a home living room, or a community early-intervention center. Goals center on building joint attention (the ability to share focus on an object or event with another person) and teaching early requesting, such as reaching toward a desired item or exchanging a picture card.
By school age, sessions become more structured. A child might work at a table with the SLP for 20 to 30 minutes within the school day, practicing phrase building, turn-taking in conversation, or reading comprehension tied to social scenarios. Goals evolve to include longer utterances, social communication skills like commenting and asking questions, and functional literacy that supports independence.
Evidence-Based Frameworks Worth Knowing
Three frameworks have accumulated meaningful research support for young autistic children.
Naturalistic Developmental Behavioral Interventions (NDBI): These approaches blend developmental science with behavioral teaching strategies inside natural play routines. An SLP using an NDBI model might sit across from a toddler at a toy farm, wait for the child to look at the horse, then model "horse go!" right at the moment of interest. Research reviews describe moderate to strong evidence for gains in social communication, language, and adaptive functioning.1 Typical SLP-led intensity is one to two hours per week, supplemented by parent coaching so that strategies carry into everyday life.
JASPER (Joint Attention, Symbolic Play, Engagement, and Regulation): A specific NDBI approach, JASPER zeroes in on helping children coordinate attention with a communication partner, expand symbolic play (pretending a block is a phone, for example), and regulate emotions during interaction.2 Sessions look playful and child-directed, but the clinician is carefully scaffolding each skill.
Hanen More Than Words: Rather than working directly with the child in most sessions, this parent-training program coaches caregivers of children roughly two to five years old to become more responsive communication partners.3 The program runs across eight to ten group sessions plus three individualized coaching visits. Research shows parents do change their interaction styles, though communication gains for children have been modest and variable,4 which is why many SLPs pair this approach with direct therapy.
When Verbal Apraxia Changes the Plan
Annie's dual diagnosis of autism and verbal apraxia meant her brain struggled to plan and sequence the precise mouth movements needed for speech. For children like Annie, therapy shifts toward motor-speech programming, a method that relies on high-frequency repetition of specific sound sequences with multisensory cues (touch, visual models, rhythmic pacing). One well-supported technique, Dynamic Temporal and Tactile Cueing, calls for sessions three to five times per week because motor learning demands intensive, distributed practice.2 This explains why Annie received four hours of speech therapy weekly, a level of intensity that might seem surprising but is consistent with clinical recommendations for childhood apraxia of speech.
Goals That Grow With the Child
One of the most important things to understand is that therapy targets are not static. Early goals might focus simply on helping a child look at a caregiver and reach for a cracker. Over months and years, those goals expand to exchanging picture cards, combining two symbols on a communication device, and eventually, for some children, producing spoken words and short phrases. Later still, therapy may address narrative language, classroom participation, and social problem-solving. The thread connecting every stage is functional communication: making sure the child can express wants, share ideas, and connect with the people around them, whether through speech, a device, signs, or some combination of all three.
Questions to Ask Yourself
When you picture a successful speech therapy outcome, does that picture include a child who communicates fluently through an iPad but rarely speaks aloud?
Many SLP students and new clinicians unconsciously equate progress with verbal speech, which can lead to setting goals that prioritize talking over functional communication. Recognizing AAC as a true form of language opens the door to celebrating meaningful gains that might otherwise be dismissed.
If your child's therapist told you to focus on communication rather than speech, what would that shift feel like for you?
Parents often grieve the dream of hearing their child's voice, and redirecting that hope toward multimodal communication can feel like giving up. Understanding that communication encompasses gestures, pictures, and devices helps families celebrate every new connection their child makes, regardless of modality.
How would your therapy approach change if you knew a child might not speak until age 10, or at all?
Long timelines challenge clinicians to sustain family engagement and morale over years of incremental progress. Building goals around immediate functional communication, rather than distant speech milestones, keeps therapy relevant and reinforces that every step forward matters.
What role does a parent's grief play in the therapy room, and how can you acknowledge it without letting it derail progress?
Parents may silently mourn milestones they expected, which can influence their willingness to embrace AAC or other non-speech tools. Creating space for that grief while gently steering focus toward what the child can do today builds trust and keeps the family moving forward together.
AAC Tools: PECS, Proloquo2go, and Beyond
Will using an AAC device prevent my child from learning to talk? This concern surfaces in nearly every conversation speech-language pathologists have with parents of minimally verbal children. The answer, supported by decades of research, is reassuring: augmentative and alternative communication does not replace speech. In fact, studies consistently show that AAC often supports and accelerates verbal development by reducing communication frustration, building language foundations, and giving children a successful way to interact with others while their speech skills continue to develop.
What AAC Actually Means
Augmentative and alternative communication refers to any method that supplements or replaces spoken language. "Augmentative" means adding to existing speech; "alternative" means serving as the primary communication mode when speech is not functional. AAC ranges from low-tech picture boards and sign language to high-tech speech-generating devices and tablet applications. For children with autism and verbal apraxia like Annie, augmentative communication devices become a bridge to connection, not a barrier to speech.
Annie began with the Picture Exchange Communication System, a low-tech approach where children hand over picture cards to request items or express needs. PECS taught her the fundamental purpose of communication: that exchanging information with another person produces results. This foundation proved essential. As she grew and technology advanced, Annie transitioned to ProLoQuo2Go, an iPad application that generates spoken words when the user taps icons. By her twenties, she had also independently learned to use Google searches to explore personal interests, from Sesame Street characters to favorite foods, demonstrating how AAC skills generalize into broader digital literacy.
AAC vs. Speech Therapy: Understanding the Relationship
A common question parents ask is what distinguishes AAC from speech therapy. The answer is straightforward: AAC is a tool within the speech-language pathologist's toolkit, not a separate treatment track. SLPs remain the professionals responsible for evaluating which AAC system fits a child's motor abilities, cognitive profile, and communication goals. They select devices, customize vocabulary layouts, and train both children and families on effective use. Speech therapy sessions may simultaneously target verbal production, AAC proficiency, and the pragmatic skills needed to use either modality in real-world conversations. Families looking for a broader overview of speech therapy apps for kids may find additional context helpful when comparing tablet-based options.
Current AAC Options
Families today have more AAC choices than ever:
PECS: A structured, low-tech system using laminated picture cards. Ideal for young children or those just learning the concept of communication exchange.
Speech-generating devices: Dedicated hardware designed specifically for communication, often funded through insurance or Medicaid.
Tablet applications: ProLoQuo2Go and TouchChat are among the most widely used. These apps turn iPads into powerful communication tools with customizable vocabulary.
Hybrid approaches: Many children use a combination, keeping a simple picture board at school while using a tablet app at home.
SLPs guide families through this landscape, matching each child's strengths and needs to the right system. They also provide ongoing training, ensuring parents feel confident supporting AAC use during meals, play, and daily routines. The goal is always functional communication, however it emerges.
Every child's communication path unfolds differently, but Annie's story illustrates a pattern that speech-language pathologists often see in minimally verbal autism: years of steady, incremental work followed by moments of breakthrough. The timeline below captures key milestones across more than two decades. While no two journeys look alike, the rhythm of patient effort and meaningful progress is a theme many families will recognize.
How Parents Can Support Speech Therapy Goals at Home
Supporting speech therapy goals at home means weaving communication practice into the everyday moments you already share with your child: during meals, bath time, play, and daily routines, not adding another hour of structured drills to a packed schedule. When parents learn to use evidence-based strategies consistently, children with autism make larger gains in language and social communication. This isn't about becoming a therapist; it's about learning to respond to your child in ways that invite interaction and build skills naturally.
Evidence-Based Parent Coaching Models
Several well-researched programs show exactly how parent involvement accelerates progress. Project ImPACT (Improving Parents as Communication Teachers) teaches parents to target social communication, imitation, and play within everyday routines. Caregiver-implemented Naturalistic Developmental Behavioral Interventions (NDBIs) blend behavioral teaching with developmental science, encouraging parents to follow the child's lead, create opportunities for communication, and respond enthusiastically. The Hanen "It Takes Two to Talk" program gives parents concrete video-based feedback on how to observe, wait, and listen to their child's initiations.
Meta-analyses confirm this works: parent-implemented interventions produce a moderate effect size of 0.553 overall, with specific improvements in language and communication (0.545) and positive social behavior (0.603).1 Annie's mother built an ambitious home-based program incorporating speech, occupational, and physical therapy. While that level of intensity isn't realistic for every family, even small, focused interactions, like modeling her daughter's AAC device during a snack, mirror the skilled approach SLPs coach parents to use. The key is consistency and responsiveness, not a packed therapy schedule.
Small Shifts, Big Impact: Strategies to Start This Week
If your child's SLP hasn't yet introduced parent coaching, you can still begin with these simple, high-impact strategies:
Narrate your daily routines: Describe what you're doing as you do it, using simple, repetitive language. For example, "Mommy is pouring milk. Let's pour the milk." This provides a language model without demanding a response.
Honor all communication attempts: Respond to gestures, sounds, facial expressions, and AAC use as meaningful communication. When your child points to a cup, say, "You want a drink! Let's get your cup," reinforcing the link between communication and getting needs met.
Practice AAC targets during motivating activities: If your child uses a communication device or picture cards, point to specific symbols while speaking aloud during meals, play, or bath time. For instance, model "more," "eat," or "all done" during a favorite snack.
Create communication temptations: Put a desired toy in sight but out of reach, or pause a familiar song at a favorite part. Wait expectantly. These gentle provocations encourage your child to initiate a request, a look, or a vocalization to continue the activity.
Coaching, Not Just Worksheets: The SLP's Role
Research underscores that handing parents a worksheet is not enough. Effective parent coaching requires SLPs to embed teaching directly into therapy sessions. In NDBI models, therapists strive for a parent fidelity threshold of around 75%,2 meaning they observe, model, and give in-the-moment feedback until the parent uses strategies accurately. When SLPs coach parents during real interactions rather than lecturing, children show measurable gains in autism speech therapy techniques and language.
Annie's story illustrates this beautifully. Her SLP didn't just work with Annie; she equipped the family to continue that work at home, gradually introducing AAC tools like PECS and ProLoQuo2Go. The result was a child who, at age 24, speaks in three- to four-word phrases and uses an iPad to express herself. Progress was slow, nonlinear, and deeply tied to her mother's daily commitment. For parents, the takeaway is clear: you are your child's most important communication partner, and every responsive interaction is a building block toward functional communication.
Realistic Timelines: How Long Does Speech Therapy Take to Work for Autism?
Speech therapy for autistic children does not run on a predictable clock, and any provider who promises one is not being honest with the family. The evidence points to wide variability, meaningful late gains, and outcomes that depend heavily on what we choose to measure.
What the Research Actually Shows
Roughly 25 to 30 percent of autistic children are non-speaking or minimally verbal.1 Among that group, a landmark 2013 longitudinal study found that about 70 percent gained phrase speech by age 8, and 47 percent achieved fluent speech in the same window.2 The remaining 30 percent stayed minimally verbal into later childhood. Most speech gains, when they happen, cluster between ages 4 and 8, with nonverbal IQ and social engagement emerging as the strongest predictors.2 Children with average nonverbal IQ tend to reach phrase speech roughly six months earlier than peers with lower nonverbal cognition.
Annie's timeline sits outside that curve. Her first words ("mama," "want mama," "no") arrived just after her tenth birthday, and at 24 she speaks in 3 to 4 word phrases while continuing to use her iPad.3 Her story is a direct rebuttal to the outdated cutoff that children who are not speaking by age 5 never will. Late talker therapy research confirms that language emergence after age 5 is possible, though it remains the minority path.
Co-Occurring Conditions Shift the Timeline
Annie also has verbal apraxia, which slows the rate of speech improvement even when a child is highly motivated to communicate.1 About 60 percent of autistic children with co-occurring intellectual disability show moderate to severe language problems, and a higher proportion of that group remains minimally verbal long term.4 Sensory processing differences, motor planning challenges, and attention profiles all stretch expected timelines further. Parents deserve to hear this plainly rather than be handed a generic 6 to 12 month projection.
Measure Functional Communication, Not Just Words
Much of the competitor content on autism and speech therapy leans on "recovery" language that overstates what most families experience. A more honest frame: Annie learning to blow out her eighth birthday candle was a genuine oral-motor milestone. So was her first independent Google search for a Sesame Street character. AAC use does not impede spoken language and can actually facilitate it, per 2018 Cochrane evidence.5 Success is functional communication, in whatever modality gets the child heard.
Did You Know?
At 24, Annie speaks in three to four word phrases and uses her iPad to Google favorite Sesame Street characters, order food, and navigate her world. That is communication success. SLPs must help families redefine what finding a voice means: functional, meaningful communication takes many forms, and speech is only one of them.
When Your Child Is Minimally Verbal: Navigating Grief and Hope
Around Annie's fifth birthday, her mother confronted a painful realization: her daughter might never speak. This experience, often described in clinical literature as ambiguous grief, is well documented among parents of disabled children. Unlike grief tied to a single loss, ambiguous grief lacks a clear endpoint. There is no closure, because the child is present and growing, yet the future a parent once imagined may look profoundly different from the one unfolding.
A Grief That Resurfaces
What makes this emotional reality so difficult is its recurring nature. Ambiguous grief does not follow a neat timeline. It resurfaces at milestone ages: the moments when peers are starting kindergarten, receiving first communions, learning to read aloud, or walking across a graduation stage. Each of these occasions can reopen the wound, even for parents who have made genuine peace with their child's communication profile. Annie's mother experienced this cycle for years, mourning an imagined version of her daughter's life while simultaneously fighting for the real one.
Hope and grief are not opposites in this context. They coexist, sometimes within the same hour. Annie eventually spoke her first words, "mama," "want mama," and "no," shortly after her tenth birthday, years after many professionals might have shifted expectations entirely.1 That timeline underscores a truth that families and clinicians alike need to internalize: communication breakthroughs can happen well beyond early childhood.
What SLPs Can Do
Speech-language pathologists occupy a unique position in a family's life during these years. They are often the professionals parents see most frequently, sometimes multiple times per week. That sustained relationship creates both an opportunity and a responsibility. SLPs can acknowledge a parent's grief without resorting to toxic positivity, phrases like "everything happens for a reason" or "just stay positive" that dismiss real pain. Instead, effective clinicians help parents reframe their goals. The shift from "my child will talk" to "my child will communicate" is not a concession. It is an expansion, one that opens the door to autism speech therapy techniques, gestural language, and other modalities that give a child genuine agency.
SLPs can also connect families to peer support networks, where parents who have navigated similar journeys offer perspective that no clinical advice can replicate. Hearing from another parent who mourned, adapted, and found joy in unexpected milestones can be transformative.
The Teletherapy Option for Overwhelmed Families
For families managing intensive therapy schedules or living in areas with limited access to specialized providers, teletherapy has emerged as a meaningful option. A 2023 systematic review and meta-analysis of 21 studies found that telehealth-delivered social communication interventions for children on the autism spectrum produced a large effect size for pragmatic language outcomes (Hedges' g of 0.89), a statistically significant result.2 Separately, a review of six studies examining parent-mediated telehealth interventions reported higher parent knowledge, satisfaction, and compliance compared to standard in-person approaches, along with improvements in children's social skills, communication, and positive affect.3
Parents of minimally verbal autistic children who participated in telepractice-based education programs described the experience as convenient, practical, and less stressful.3 Research also found that parent training fidelity remained high in telehealth formats, suggesting that caregivers can learn and implement strategies effectively through a screen. Notably, parents reported reduced stress and improved family situations when telepractice was part of the intervention model, though the reduction in stress did not reach statistical significance across all reviewed studies.3
Teletherapy does not replace the relationship between an SLP and a child, but it can reduce the logistical burden that contributes to caregiver burnout: fewer drives across town, fewer missed work hours, and fewer siblings shuffled between waiting rooms. For a parent already navigating ambiguous grief, removing even one source of daily friction matters. While formal research on integrating grief support into telehealth speech therapy sessions remains limited, the format itself, delivered in the family's own home, may naturally create a more comfortable space for these conversations to unfold.3
How SLPs Collaborate With ABA Therapists, OTs, and Schools
Annie's mother built a comprehensive home-based ABA program that incorporated speech, occupational, and physical therapy while Annie attended Devereux CARES, a specialized autism center. This multidisciplinary model is the gold standard for children with complex communication needs. When therapy teams work in parallel rather than partnership, however, children often receive conflicting cues, fragmented goals, and slower progress. Strong interprofessional collaboration requires clear roles, shared language, and genuine respect for each discipline's expertise.
The SLP's Specific Role on the Team
On a multidisciplinary autism team, the SLP typically leads communication assessment and intervention planning. In Annie's case, the SLP likely introduced PECS, later transitioned her to ProLoQuo2Go, and trained the family and ABA therapists to honor and reinforce those communication methods across all settings. The board-certified behavior analyst (BCBA) then embeds those systems into the child's ABA program, using reinforcement schedules to increase spontaneous use of the AAC device. SLP vs occupational therapy roles often overlap here: occupational therapists address sensory and motor barriers that can impede communication, such as oral-motor planning deficits (apraxia), tactile defensiveness that makes PECS hand-over-hand prompting aversive, or core weakness that affects breath support for vocalization. Physical therapists ensure positioning supports access to AAC devices and participation in communication-rich activities.
Navigating ABA and SLP Philosophical Differences
A common tension arises when ABA programs emphasize discrete-trial verbal imitation ("Say 'ball'") while SLPs prioritize naturalistic, child-led communication. Annie's journey illustrates the risk of pressuring speech: she did not speak until age 10, yet she became a functional communicator years earlier through AAC devices. Effective teams negotiate complementary goals by asking, "What does this child need to communicate right now, and what method will work fastest?" rather than defaulting to speech as the only valid outcome. SLPs should advocate for communication over articulation when the two are in conflict, and ABA therapists should defer to the SLP's expertise on which modality to target.
Three Practical Collaboration Tips for SLPs
Joint goal-writing: Schedule quarterly meetings where the SLP, BCBA, OT, teacher, and parents co-write a single set of functional goals. Annie's mother coordinated four hours of speech therapy per week with her home ABA program; that level of alignment requires shared targets, not parallel plans.
Shared data collection: Use a common progress-monitoring tool (Google Sheets, therapy software, or a shared notebook) so all team members track the same communication behaviors. If the SLP sees PECS generalization at school but the ABA therapist does not see it at home, the data reveal where to intensify support.
Regular team meetings with parents at the center: Invite parents to lead the agenda. Annie's mother drove her daughter's program because she knew Annie best. SLPs who position families as co-therapists rather than passive recipients see faster carryover and stronger long-term outcomes.
Lessons for Future SLPs: What Annie's Story Teaches About Family-Centered Care
What clinical skills separate effective speech-language pathologists from those who simply deliver protocols? Annie's 22-year communication journey offers five evidence-based lessons for SLP students entering the profession, grounding abstract concepts like family-centered care in real outcomes.
Introduce AAC Early, Don't Wait for Speech to Fail
Annie's mother introduced PECS when Annie was two, immediately after her autism and verbal apraxia diagnoses. The family did not wait to see if speech would emerge naturally. This decision gave Annie a functional communication system years before her first spoken words at age 10. Research supports early AAC implementation: it does not inhibit speech development and often facilitates it. SLP students should learn to recommend AAC tools during initial evaluations, not as a last resort after years of frustration.
Coach Parents as Active Communication Partners
Annie received four hours of formal speech therapy each week, but her mother also built a home-based program integrating speech goals into daily routines. Effective SLPs train caregivers to use modeling, prompting, and reinforcement strategies during meals, play, and transitions. Family-centered care, as defined in ASHA's scope of practice, is not a soft skill or optional add-on. It is a clinical competency. SLPs who view parents as passive observers miss opportunities to multiply therapy hours and generalize skills across environments.
Set and Revisit Goals Across Developmental Stages
Annie's communication needs at age 2 (establishing a yes/no system), age 8 (learning to blow out candles, a motor speech milestone), age 10 (producing first words), and age 24 (using 3-4 word phrases plus iPad-based AAC) required different goals and tools. SLPs must resist static treatment plans. Regular reassessment and collaboration with families ensure goals remain relevant as the child grows. SLP graduate student clinical practicum experiences are an ideal time to practice this kind of iterative goal-setting under supervision.
Honor All Forms of Communication
Annie's mother mourned around her daughter's fifth birthday, believing Annie would never speak. Yet Annie communicates effectively today through multimodal means: spoken phrases, ProLoQuo2Go, and independent Google searches to explore interests. SLPs should celebrate functional communication in all its forms, helping families shift focus from talking to connecting.
Support the Emotional Wellbeing of the Family
Grief, hope, and persistence marked Annie's mother's experience. The SLPs who made the biggest difference listened to the family's fears, validated their emotions, and adapted treatment plans accordingly. SLP career settings shape how much time clinicians have to invest in this kind of family partnership, so students should consider their preferred environment carefully. Graduate programs should develop this capacity for empathy and flexibility alongside technical skills.
For students preparing for careers in speech-language pathology, Annie's story illustrates that clinical excellence requires more than articulation drills and language samples. It demands partnership, adaptability, and a commitment to the family's long-term journey.
Frequently Asked Questions About Speech Therapy for Autistic Children
Families navigating autism and communication challenges often share similar questions. The answers below draw on the key themes explored throughout this article, including Annie's journey from a nonverbal toddler to a young adult who communicates through both speech and technology.
What does speech therapy look like for a child with autism?
Sessions are tailored to each child's needs and may include play-based activities, picture cards, modeling language, and technology-assisted communication. Annie, for example, received four hours of speech therapy per week alongside occupational and physical therapy. An SLP sets individualized goals that range from basic requesting to conversational turn-taking, adjusting the approach as the child develops new skills.
How long does speech therapy take to work for autism?
There is no universal timeline. Some children show progress within months, while others, like Annie, reached major milestones years into therapy. Annie spoke her first words shortly after her tenth birthday, more than eight years after her diagnosis. Consistent therapy, family involvement, and realistic goal-setting all influence the pace of progress. Celebrating small wins along the way helps sustain motivation.
Can a nonverbal autistic child learn to speak with speech therapy?
Some children do develop spoken language over time, even after years of being minimally verbal. Annie began using words like "mama," "want mama," and "no" after her tenth birthday and now speaks in three- to four-word phrases at age 24. However, communication success does not depend on speech alone. Many children communicate effectively through AAC tools alongside whatever verbal skills they develop.
What is the difference between AAC and speech therapy for autism?
Speech therapy is a broad clinical service that addresses all aspects of communication, including language comprehension, social interaction, and speech production. AAC (augmentative and alternative communication) is a set of tools and strategies used within speech therapy to support or replace spoken language. Annie used PECS cards first, then transitioned to ProLoQuo2Go on an iPad. AAC and speech therapy work together, not as separate paths.
How do speech therapists work with autistic children who have apraxia?
When a child has both autism and verbal apraxia, as Annie did, the SLP targets motor planning for speech alongside broader communication goals. Therapy may include repetitive practice of sound sequences, multisensory cues, and AAC to reduce frustration while oral-motor skills develop. Annie's journey shows that progress with apraxia can be slow but meaningful, with breakthroughs sometimes arriving well beyond early childhood.
How can parents support speech therapy goals at home?
Parents can reinforce SLP strategies during everyday routines by modeling target words, honoring AAC use, and creating opportunities for communication. Annie's mother built a home program that incorporated ABA-based techniques alongside speech, occupational, and physical therapy. Simple actions, such as pausing before fulfilling a request so the child can practice communicating, make a significant difference over time.
Is teletherapy effective for speech therapy with autistic children?
Research supports teletherapy as a viable option for many children, though effectiveness varies with the child's age, attention span, and comfort with technology. For families in underserved areas or those managing complex schedules, teletherapy can maintain continuity of care. A parent or caregiver typically participates in the session, which can strengthen carryover of skills at home. Your SLP can help determine whether a virtual format suits your child's needs.