The 10 Most Common Speech-Language Disorders and How They're Treated
A comprehensive guide to symptoms, causes, prevalence, and evidence-based SLP treatments for children and adults.
By Benjamin Thompson, M.S., CCC‑SLPReviewed by SLP Editoral TeamUpdated August 4, 202625+ min read
Points of interest…
Apraxia, stuttering, aphasia, and dysarthria are among the ten most common speech-language disorders SLPs treat across all ages.
Children who begin speech therapy before age 5 are up to twice as likely to achieve age-appropriate communication skills.
Voice disorders affect 3 to 9 percent of the U.S. population, yet they often go undiagnosed without proper SLP screening.
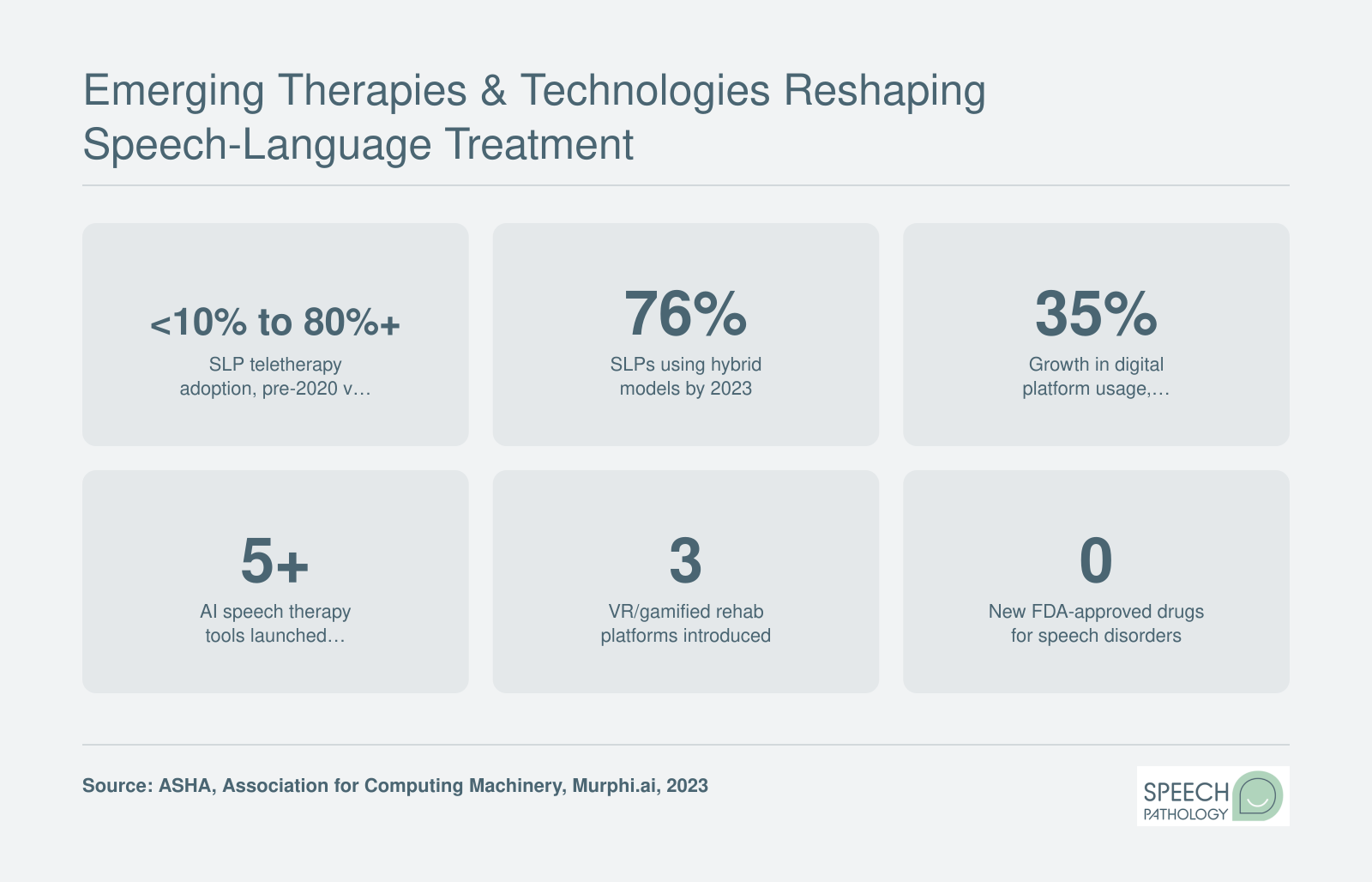
AI tools, teletherapy, and virtual reality platforms are rapidly expanding how clinicians deliver speech-language treatment.
Roughly 1 in 12 U.S. children has a speech, language, or swallowing disorder, according to the National Institute on Deafness and Other Communication Disorders. Millions of adults are affected as well, often after stroke, traumatic brain injury, or progressive neurological disease.
The clinical distinctions matter. Speech disorders involve the mechanics of sound production, fluency, or voice quality. Language disorders affect a person's ability to comprehend or formulate words and sentences. Social communication disorder sits in a broader category, covering pragmatic skills like turn-taking and interpreting context. Swallowing disorders (dysphagia) round out the SLP scope of practice, since speech-language pathologists are the primary professionals who assess and treat them.
For students entering the field, knowing where these 10 conditions overlap and where they diverge shapes everything from graduate coursework selection to clinical fellowship placement decisions. The sections below walk through each disorder's symptoms, causes, affected populations, and standard treatment approaches so you can start building that clinical foundation now.
Apraxia of Speech: Childhood & Acquired
Apraxia of speech is a motor-planning disorder, not a muscle weakness or a language comprehension problem. The brain knows what it wants to say but struggles to coordinate the precise movements of the lips, tongue, jaw, and palate needed to produce clear speech. Two distinct forms share this underlying mechanism, yet they differ sharply in who they affect and how they are managed.
Childhood Apraxia of Speech (CAS)
CAS is present from birth, though red flags typically become noticeable between ages two and three, when a child's spoken vocabulary should be expanding rapidly. Because CAS disrupts the planning and sequencing of speech movements rather than the muscles themselves, it can be tricky to distinguish from other speech sound disorders in very young children.
Common signs to watch for include:
Inconsistent error patterns: The same word may be produced differently each time the child attempts it.
Groping movements: Visible searching or struggling with the lips and jaw before or during speech attempts.
Difficulty with longer or more complex words: A child may say a short word correctly but break down when attempting multisyllabic words.
Limited babbling history: Parents sometimes report that the child was unusually quiet as an infant.
Vowel distortions: Unlike many articulation disorders that primarily affect consonants, CAS often distorts vowels as well.
If a child is not combining words by age two or remains largely unintelligible to familiar listeners by age three, a referral for a comprehensive speech language evaluation is warranted.
Acquired Apraxia of Speech
Acquired apraxia appears in adolescents or adults following neurological events such as stroke, traumatic brain injury, or progressive neurological disease. The hallmark symptoms mirror those seen in CAS (inconsistent errors, effortful groping, breakdowns on longer utterances), but the onset is sudden or degenerative rather than developmental. Acquired apraxia frequently co-occurs with aphasia, which can complicate both diagnosis and treatment planning.
Prognosis varies. Adults who develop apraxia after a single stroke often recover a significant degree of functional communication, especially with early, intensive therapy. In progressive conditions, the goal shifts toward maintaining communication ability as long as possible and introducing augmentative strategies.
Treatment Approaches
Because apraxia is rooted in motor planning rather than knowledge of language, therapy emphasizes repetitive, structured practice of speech movements. Several evidence-based speech therapy techniques are commonly used by speech-language pathologists:
PROMPT (Prompts for Restructuring Oral Muscular Phonetic Targets): A tactile-kinesthetic method in which the clinician uses gentle touch cues on the client's face, jaw, and mouth to guide articulatory movements.
Dynamic Temporal and Tactile Cueing (DTTC): A highly systematic technique that pairs auditory models with tactile prompts, gradually fading cues as the client gains control.
Intensive practice schedules: Research consistently shows that individuals with apraxia benefit from high-frequency sessions, typically three to five times per week, rather than the once-weekly schedule that may suffice for other speech sound disorders.
CAS often requires a longer course of therapy than a straightforward articulation disorder. Families should be prepared for a commitment spanning months or even years, though gains tend to be steady when therapy is frequent and well-structured.
Living With Apraxia
Apraxia can be isolating, particularly for children who understand language well but cannot express themselves. Augmentative and alternative communication tools, ranging from simple picture boards to speech therapy apps for kids, provide a bridge while verbal skills develop. For students exploring speech-language pathology as a career, apraxia cases offer a vivid example of how evidence-based motor-learning principles translate directly into measurable client progress, making this one of the most rewarding areas of clinical practice.
Stuttering & Other Fluency Disorders
Fluency disorders disrupt the natural rhythm and flow of speech, and stuttering is by far the most recognized among them. For students building careers in speech-language pathology, understanding the different origins of fluency breakdowns is essential to accurate assessment and effective treatment planning.
Types of Stuttering
Not all stuttering shares the same cause, and clinicians must differentiate among three primary types:
Developmental stuttering: The most common form, typically emerging between ages 2 and 6. Roughly 5% of children experience developmental stuttering at some point during early speech and language development.
Neurogenic stuttering: An acquired form that appears after a stroke, traumatic brain injury, or other neurological event. The disruptions tend to occur across all speaking contexts rather than fluctuating with emotional state.
Psychogenic stuttering: The rarest type, linked to emotional trauma or psychological distress. Onset is usually sudden, and the pattern may not match the hallmark features of developmental or neurogenic stuttering.
Other fluency disorders such as cluttering (characterized by rapid or irregular speech rate and collapsed syllables) also fall within an SLP scope of practice and require their own assessment protocols.
The Emotional and Social Toll
Fluency disorders carry weight far beyond the speech signal itself. Children who stutter may withdraw from classroom participation, while adults often develop avoidance behaviors, substituting words or sidestepping situations that feel risky. Workplace stigma remains a real barrier: research consistently shows that listeners may perceive people who stutter as less competent or less confident, despite no basis in fact.
Anxiety tied to speaking can compound the disorder over time, creating a cycle in which fear of stuttering increases the frequency and severity of disfluencies. Building empathy for this lived experience is a critical part of clinical training, because effective therapy addresses the whole person, not just the speech pattern.
Evidence-Based Treatments
SLPs draw on several well-supported approaches depending on the client's age and needs:
Lidcombe Program: A behavioral treatment designed for preschool-age children. Parents deliver structured feedback in everyday conversations, and research supports its effectiveness in reducing stuttering frequency during the critical early years.
Fluency shaping: Teaches techniques such as gentle onset of voicing, slow speech rate, and controlled breathing to produce smoother speech. This approach is commonly used with older children and adults.
Stuttering modification: Rather than eliminating disfluencies entirely, this method helps clients stutter more easily and with less tension, reducing the struggle that often accompanies speech blocks.
Cognitive behavioral therapy (CBT): Increasingly used as an adjunct to direct speech therapy, CBT targets the anxiety, negative self-talk, and avoidance patterns that can sustain a fluency disorder even when speech techniques improve.
Why Early Intervention Still Matters
The encouraging reality is that approximately 75 to 80 percent of children who stutter will recover naturally, often within a year or two of onset. That statistic, however, should not inspire a wait-and-see approach. For the remaining 20 to 25 percent, early identification and intervention significantly improve long-term outcomes. Research suggests that therapy initiated during the preschool years, when the brain's neural pathways for speech are most plastic, yields the strongest gains.
As a future SLP, recognizing the signs of persistent stuttering early and connecting families with appropriate services can change the trajectory of a child's communication development and social confidence for years to come. Thorough SLP evaluation and treatment planning helps ensure families receive timely, individualized support.
Questions to Ask Yourself
Does your child consistently substitute or drop certain sounds after age 4?
Most children master basic speech sounds by age 4 to 5. Persistent substitutions, like saying "wabbit" for "rabbit," may signal an articulation or phonological disorder that responds best to early intervention with a speech-language pathologist.
Has an adult family member started struggling to find words or speak clearly after a stroke, brain injury, or other health event?
Sudden difficulty retrieving words or slurred speech in an adult often points to aphasia or dysarthria. Identifying these signs quickly helps determine whether the person needs a speech-language pathologist, a neurologist, or both.
Are the difficulties mainly with producing sounds, forming sentences, or using language socially?
This distinction matters because each category calls for a different evaluation approach. Sound-production issues suggest a motor speech disorder, sentence-level problems may indicate a language disorder, and social-use challenges often relate to pragmatic or social communication disorder.
Do you notice these patterns across settings, or only in specific situations like school or stressful conversations?
Context-dependent difficulties, such as stuttering that worsens under pressure, can look different from consistent impairments. Documenting when and where symptoms appear gives a clinician critical information for accurate diagnosis and treatment planning.
When a stroke or traumatic brain injury (TBI) disrupts the neural pathways that power speech and language, the consequences can be life-altering. Dysarthria, aphasia, and cognitive-communication disorders are the three adult-onset conditions every future SLP and caregiver should understand. They are also the stroke and TBI speech conditions that many popular resources gloss over, even though they collectively affect millions of Americans.
Dysarthria: When Speech Muscles Falter
Dysarthria occurs when the muscles used for speech become weak, slow, or uncoordinated. The result is slurred, imprecise, or abnormally soft speech that can be difficult for listeners to understand. Causes include stroke, Parkinson's disease, multiple sclerosis, amyotrophic lateral sclerosis (ALS), and brain injury. Among inpatient stroke survivors, roughly 26 percent present with dysarthria during the acute or subacute phase.1 In people living with Parkinson's disease, estimates suggest that 50 to 90 percent will experience some degree of dysarthria over the course of their illness.
One of the most well-researched treatment approaches is Lee Silverman Voice Treatment, commonly known as LSVT LOUD. Originally developed for individuals with Parkinson's disease, LSVT LOUD trains patients to produce speech with greater vocal effort and improved loudness. The protocol is intensive, typically delivered in 16 sessions over four weeks, and has demonstrated lasting improvements in vocal volume and speech intelligibility.
Aphasia: Language Lost After Stroke
Aphasia is a language impairment, not a speech-muscle problem. It affects the ability to produce or comprehend spoken and written language. Approximately 2 million Americans currently live with aphasia2, and roughly 180,000 new cases are diagnosed each year.3 Between 25 and 40 percent of stroke survivors develop aphasia, and about 38 percent of stroke patients present with aphasia at onset.3 By three months post-stroke, around 25 percent still have measurable aphasia. The risk also increases with age: about 15 percent of stroke survivors under 65 develop the condition, compared to 43 percent of those over 85.3
Clinicians categorize aphasia into several types:
Broca's aphasia: Individuals understand language relatively well but produce speech with great effort, often in short, halting phrases.
Wernicke's aphasia: Speech flows easily but may be filled with nonsensical or substituted words, and comprehension is significantly impaired.
Global aphasia: Both production and comprehension are severely affected, typically resulting from extensive damage to the language-dominant hemisphere.
A less common variant, primary progressive aphasia (PPA), is a neurodegenerative condition rather than a stroke-related one. Roughly 13,400 people in the United States live with PPA, with an incidence rate of about 0.56 per 100,000.4 Despite its prevalence, public awareness of aphasia remains surprisingly low. Studies suggest that only 40 to 68 percent of U.S. adults have even heard of the condition.5
Evidence-based aphasia treatments include constraint-induced language therapy, which encourages patients to rely on verbal expression rather than gestures or other compensatory strategies, and script training, in which patients rehearse functional, personally relevant dialogues until delivery becomes more fluent and automatic.
Cognitive-Communication Disorders: The Hidden Impact of TBI
Cognitive-communication disorders arise when a traumatic brain injury or other neurological event disrupts the cognitive processes that underpin communication. Rather than affecting the mechanics of speech or the grammar of language, these disorders impair attention, memory, organization, problem-solving, and executive function. A person may speak clearly and use correct grammar yet struggle to follow a conversation, stay on topic, or interpret social cues.
SLPs address cognitive-communication disorders through compensatory strategy training. This approach teaches individuals to use external aids such as planners, checklists, and smartphone reminders, while also practicing internal strategies like self-cueing and structured self-monitoring during conversation. Group therapy settings can be especially valuable, offering real-world practice in turn-taking, topic maintenance, and social pragmatics.
Why These Disorders Deserve More Attention
For students exploring speech-language pathology as a career, adult neurogenic communication disorders represent a significant and growing area of clinical need. An aging population means more strokes, more neurodegenerative diagnoses, and more demand for SLPs trained in evidence-based adult rehabilitation. If you are drawn to this area, consider learning how to become a medical SLP so you can build the skills these patients urgently need.
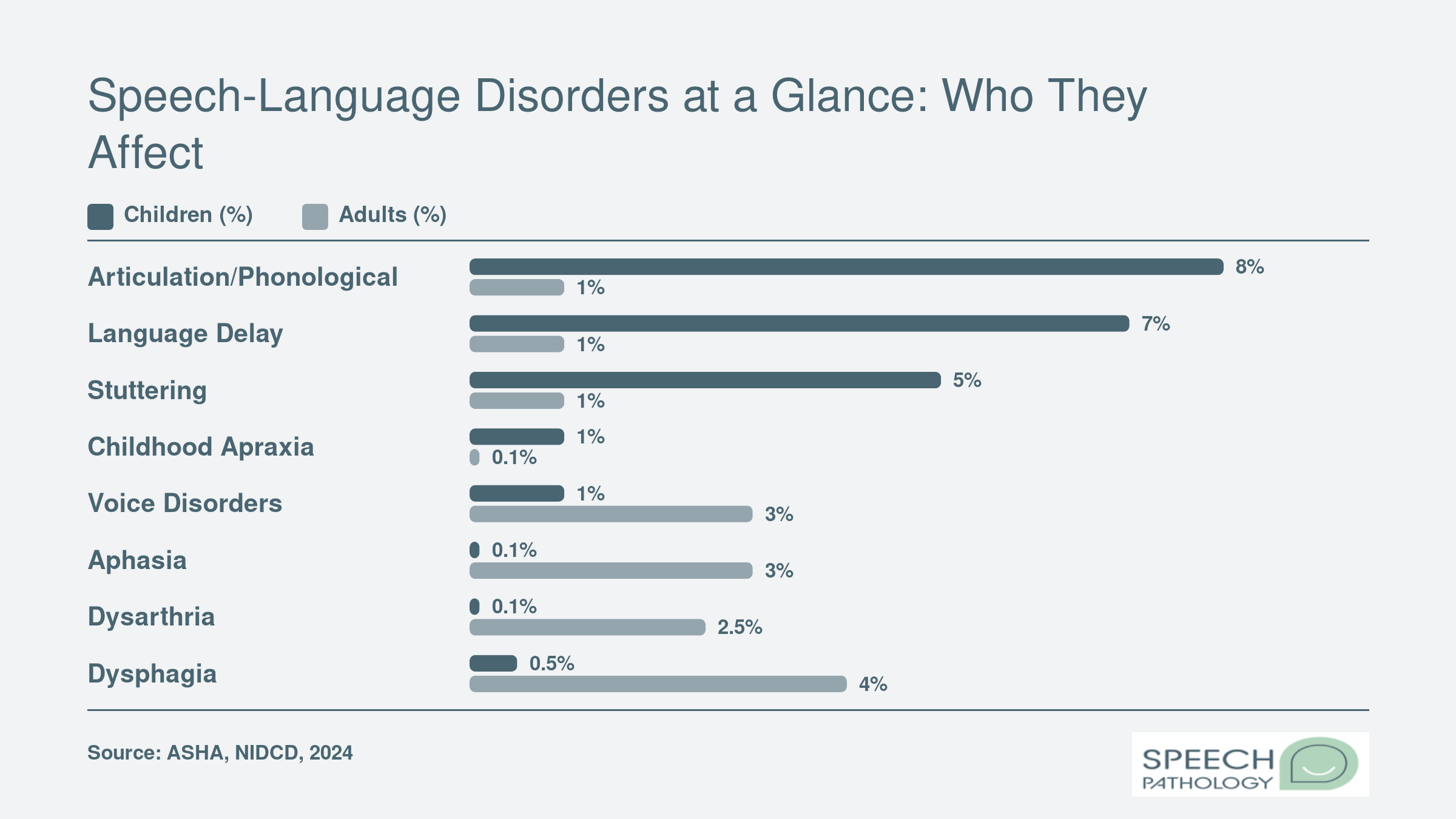
Speech-Language Disorders at a Glance: Who They Affect
Not all speech-language disorders are equally common, and prevalence varies dramatically by age group. Articulation and phonological disorders top the charts in pediatric caseloads, while aphasia and dysarthria are far more prevalent among adults, particularly after stroke or neurological injury. Understanding these patterns helps future SLPs anticipate the populations they will serve most often.
Voice Disorders & Spasmodic Dysphonia
Voice disorders affect an estimated 3 to 9 percent of the U.S. population at any given time, making them one of the most common categories of communication impairment that speech-language pathologists encounter. These conditions range from mild hoarseness caused by vocal overuse to complex neurological conditions that alter the voice for life. Understanding the distinction between functional and neurological voice disorders is essential for anyone pursuing a career in speech-language pathology.
Functional Voice Disorders: Causes and Risk Factors
Functional voice disorders develop primarily from vocal misuse, overuse, or poor vocal hygiene rather than structural or neurological abnormalities. The most familiar examples include vocal nodules (sometimes called "singer's nodes"), vocal polyps, and contact ulcers. These conditions arise when the vocal folds endure repeated mechanical stress, leading to tissue changes that disrupt normal vibration.
Certain professions carry elevated risk because they demand sustained, high-volume voice use:
Teachers: Studies consistently identify classroom educators as one of the highest-risk groups for voice disorders.
Singers and performers: Prolonged rehearsal schedules and performance demands place extraordinary strain on the vocal mechanism.
Coaches and fitness instructors: Shouting over background noise in gyms or on athletic fields contributes to chronic vocal fold irritation.
Clergy and public speakers: Extended speaking engagements with limited vocal rest compound tissue fatigue over time.
The good news is that functional voice disorders are often highly treatable and, in many cases, fully reversible with appropriate intervention.
Neurological Voice Disorders: Spasmodic Dysphonia and Vocal Fold Paralysis
Neurological voice disorders originate from disruptions in the nervous system's control of the laryngeal muscles. Spasmodic dysphonia, a focal dystonia, causes involuntary spasms of the vocal folds during speech. It most commonly appears in middle-aged adults, typically between the ages of 30 and 50, and affects women more frequently than men. Patients often describe a strained, strangled voice quality (adductor type) or a breathy, weak voice (abductor type) that can fluctuate unpredictably.
Vocal fold paralysis, another neurological voice disorder, results from damage to the nerves supplying the larynx. It can stem from surgical complications, viral infections, tumors, or stroke.
Treatment Approaches
SLPs play a central role in treating both categories of voice disorders, though the strategies differ considerably.
For functional disorders, voice therapy is the first line of treatment and often the only intervention needed. Common therapeutic techniques include:
Resonant voice therapy: Teaches patients to produce voice with minimal vocal fold collision, reducing tissue trauma.
Vocal function exercises: A structured program of sustained phonation and pitch glides designed to strengthen and balance the laryngeal muscles.
Vocal hygiene education: Addresses contributing behaviors such as throat clearing, dehydration, and speaking in noisy environments.
Many of these approaches align with broader speech therapy techniques that SLPs apply across disorder categories. For spasmodic dysphonia, Botox (botulinum toxin) injections into the affected laryngeal muscles remain the primary management strategy. These injections temporarily weaken the muscles responsible for involuntary spasms, restoring smoother voice production for roughly three to four months per treatment cycle. Emerging surgical options, including selective laryngeal denervation and reinnervation procedures, show promise for longer-lasting relief, though they are not yet universally available.
Long-Term Prognosis
One of the most frequent questions patients and families ask is whether full recovery is possible. For functional voice disorders, the prognosis is encouraging. Many patients experience complete resolution of symptoms with consistent voice therapy and behavioral changes, often within weeks to a few months.
Spasmodic dysphonia, by contrast, is a chronic condition that is managed rather than cured. However, this distinction does not mean patients are without options. Most individuals with spasmodic dysphonia maintain a functional, communicative voice through ongoing Botox treatments. Quality of life improves significantly with consistent management, and advances in surgical techniques continue to expand the possibilities for longer intervals between interventions.
For students exploring speech-language pathology as a career, voice disorders represent a rewarding clinical specialty that blends knowledge of anatomy, neurology, and behavioral therapy. Reliable speech language pathology assessment tools can help clinicians pinpoint the nature and severity of a voice disorder, guiding more targeted treatment plans.
Articulation & Phonological Disorders in Children
Speech sound disorders are among the most common reasons children are referred to a speech-language pathologist, yet the term covers two distinct clinical categories. Understanding the difference between articulation disorders and phonological disorders is essential for future SLPs, because the distinction drives treatment planning from the very first session.
Articulation vs. Phonological Disorders
An articulation disorder involves difficulty producing specific speech sounds. A child might distort, substitute, or omit individual sounds, such as replacing /r/ with /w/ ("wabbit" for "rabbit") or producing a lateral lisp on /s/. The challenge is motor in nature: the tongue, lips, or jaw are not moving to the right place at the right time.
A phonological disorder, by contrast, is a pattern-based problem. Rather than struggling with one sound, the child applies systematic simplification rules to groups of sounds. Common patterns include fronting (replacing back sounds like /k/ with front sounds like /t/, so "cat" becomes "tat"), stopping (replacing fricatives with stops), and cluster reduction ("spoon" becomes "poon"). These patterns are normal in very young children but become clinically significant when they persist past expected developmental milestones.
The 3-1 Screening Rule
SLPs frequently reference a practical benchmark known as the 3-1 rule: by age 3, a child's speech should be roughly 75 percent intelligible to unfamiliar listeners. This does not mean every sound is perfect. It means that a stranger, such as a neighbor or store clerk, should be able to understand most of what the child says. When intelligibility falls well below that threshold, it signals that a professional evaluation is warranted rather than a "wait and see" approach.
By age 4, intelligibility should climb to approximately 90 to 100 percent for familiar and unfamiliar listeners alike, even if a few later-developing sounds (like /r/, /l/, and /th/) are still emerging.
Evidence-Based Treatment Approaches
Once a diagnosis is made, SLPs choose from several well-established therapeutic frameworks that reflect evidence-based practice in speech-language pathology:
Traditional articulation therapy (Van Riper approach): Targets one sound at a time through a structured hierarchy, moving from isolation to syllables, words, sentences, and finally conversational speech. This method works well for motor-based articulation errors.
Cycles approach: Designed specifically for phonological disorders, this method rotates through targeted sound patterns over set time intervals rather than drilling a single sound to mastery. It is especially effective for children with multiple pattern errors.
Minimal pairs therapy: Presents word pairs that differ by only one sound (e.g., "key" vs. "tea") to help the child recognize that sound changes carry meaning. This builds phonological awareness and motivates self-correction.
Recovery rates are encouraging. Most children with speech sound disorders resolve their errors by age 6 or 7 when they receive consistent, targeted therapy. Research consistently supports early intervention as the strongest predictor of positive outcomes.
When to Seek an Evaluation
Parents sometimes wonder whether a child will simply "grow out of it." Some sound errors do resolve with natural maturation, but certain red flags suggest an evaluation should not be delayed:
The child is frequently frustrated or avoids speaking because others cannot understand them.
Speech intelligibility is significantly below age expectations (especially below 75 percent at age 3).
Error patterns that should have disappeared by a given age are still present, such as fronting persisting past age 3.5.
There is a family history of speech or language disorders.
When in doubt, a referral costs nothing but time, and using the right SLP assessment tools can help a clinician quickly determine whether therapy is needed or whether monitoring and parent coaching will suffice. For students exploring this career, pediatric speech sound disorders represent one of the most rewarding clinical areas, combining high caseload demand with strong, measurable treatment success.
Did You Know?
Research consistently shows that starting therapy early, before age 5 for pediatric disorders and within weeks of onset for stroke-related conditions, dramatically improves outcomes across nearly every disorder on this list. Children who receive speech-language intervention early are up to 75 percent more likely to reach age-appropriate communication milestones, making timely identification one of the most powerful tools in an SLP's practice.
Language Delays, Social Communication Disorder & Dysphagia
These three conditions may seem unrelated at first glance, but they share a common thread: each falls squarely within the scope of speech-language pathology practice, and each is frequently underrecognized. Together with articulation, fluency, voice, cognitive-communication, hearing, and augmentative and alternative communication (AAC), they round out the 9 areas of speech-language pathology, sometimes called the "Big 9." Understanding all nine helps future clinicians appreciate the true breadth of the profession.
Mixed Receptive-Expressive Language Delay
Language delays are the single most common reason children are referred to a pediatric speech language pathologist. Mixed receptive-expressive language disorder involves difficulty both understanding spoken language and using it to communicate. Symptoms in young children include a limited vocabulary for their age, trouble following multi-step directions, short or grammatically incomplete sentences, and difficulty retelling a story in logical order.
This condition frequently co-occurs with learning disabilities such as dyslexia, which can complicate diagnosis and treatment planning. Parents often ask whether the disorder can be "cured." The honest answer is that most children make significant, measurable progress with intervention, but severe cases may not resolve entirely. The goal is functional communication, not perfection.
Expressive language disorder treatment typically relies on structured language intervention strategies. These include:
Modeling: The clinician demonstrates target language forms in natural conversation so the child can absorb correct grammar, vocabulary, and sentence structure.
Milieu teaching: Therapy is embedded in everyday routines and play, capitalizing on moments when the child is motivated to communicate.
Focused stimulation: The SLP repeatedly exposes the child to specific language targets without demanding imitation, building comprehension before production.
Social communication disorder (SCD) was formally added to the DSM-5 in 2013 to describe individuals who struggle with the social use of language, such as taking turns in conversation, adjusting speech for different listeners, and understanding nonliteral language like sarcasm or idioms, without meeting the full diagnostic criteria for autism spectrum disorder.
The distinction from autism is important: SCD does not include the restricted, repetitive behaviors that characterize autism. Before its addition to the DSM-5, many of these individuals went undiagnosed or were misclassified, leaving them without targeted support. SLPs treat SCD through social skills groups, video modeling, role-play scenarios, and direct instruction in conversational rules.
Dysphagia: Why SLPs Treat Swallowing
It surprises many students to learn that swallowing disorders fall within the SLP scope of practice, yet dysphagia is one of the most medically critical conditions clinicians manage. Swallowing and speech share overlapping anatomy (the tongue, pharynx, larynx, and surrounding muscles), which is precisely why SLPs are trained to evaluate and treat both. For students interested in this clinical setting, a career as a hospital speech pathologist often involves significant dysphagia caseloads.
Dysphagia most commonly affects older adults, individuals recovering from stroke, and patients who have undergone head and neck cancer treatment. Aspiration, where food or liquid enters the airway, can lead to pneumonia and other serious complications. Standard treatment approaches include:
Diet modification: Adjusting food textures and liquid thickness to reduce aspiration risk.
Swallowing exercises: Targeted muscle-strengthening routines such as effortful swallows, the Mendelsohn maneuver, and tongue resistance exercises.
Neuromuscular electrical stimulation (VitalStim): A modality that delivers low-level electrical currents to throat muscles during swallowing exercises, aiming to retrain muscle coordination.
For students exploring SLP careers, understanding the full scope of practice, from pediatric language delays to adult dysphagia management, is essential for choosing the clinical settings and coursework that align with your professional goals.
Treatment Success Rates & What to Expect From Therapy
One of the biggest questions future speech-language pathologists hear from clients and families is straightforward: will therapy actually work? The short answer is yes, but the details matter. Outcomes vary widely depending on the specific disorder, the person's age at onset, overall severity, and how consistently therapy is delivered. This section fills a gap you will not find on most competitor pages: a side-by-side look at what the research tells us about improvement rates, timelines, and costs.
Comparing Outcomes Across the 10 Most Common Disorders
The table below draws on published meta-analyses and outcome data to give you realistic benchmarks.123
Disorder
Typical Frequency
Avg. Treatment Duration
Approx. Improvement Rate
Child vs. Adult Prognosis
Apraxia of Speech
2-3 sessions/week
20-40 sessions
60-80%
Children respond well with intensive early therapy; acquired adult apraxia varies by lesion severity
Stuttering (Preschool)
2-3 sessions/week
3-12 months
75-80%
Preschoolers have the highest natural recovery and treatment success rates
Stuttering (School-age/Adult)
1-2 sessions/week
6-24 months
60-65%
Improvement is common, but complete fluency is less likely than in younger children
Dysarthria
2-3 sessions/week
Varies widely
Depends on underlying condition
Children with developmental causes may see steady gains; adults with degenerative conditions focus on maintaining function
Aphasia
2-3 sessions/week
Months to years
~40% achieve significant recovery
Rare in children; adult prognosis depends heavily on stroke severity and time to treatment
Cognitive-Communication Disorders
1-3 sessions/week
Months to years
Varies by etiology
More common in adults after TBI or dementia; children with TBI may recover more quickly
Voice Disorders (Functional)
1-2 sessions/week
4-8 weeks
70-85%
Similar prognosis across ages when compliance is high
Voice Disorders (Neurological)
1-2 sessions/week
Ongoing
~60%
Adults are more commonly affected; progress depends on disease trajectory
Articulation/Phonological Disorders
3 sessions/week
15-20 sessions
70-90%
Primarily a childhood disorder with excellent outcomes when treated early
Language Delays
2-3 sessions/week
6-18 months
~70%
Children benefit most from early intervention; adults with acquired language issues face longer timelines
Social Communication Disorder
1-2 sessions/week
12+ months
19-30% (age under 5); 5-32% (age over 5)
Younger children show the greatest gains, particularly with structured, intensive programs
Dysphagia
Varies by setting
Weeks to months
Depends on medical cause
Children with developmental dysphagia often improve significantly; adult outcomes hinge on the underlying medical condition
A few patterns jump out. Childhood disorders, especially articulation issues and early stuttering, carry the most favorable prognosis. Neurological conditions in adults, such as aphasia and dysarthria from stroke or progressive disease, tend to require longer treatment windows and produce more variable results.
What Drives These Differences?
Three factors consistently predict how well therapy works across all ten disorders.
First, age at onset and age at treatment entry matter enormously. Children's brains are more neuroplastic, meaning they can rewire and compensate more effectively. This is why early identification is emphasized throughout speech language pathology training.
Second, therapy intensity plays a measurable role. Research supports higher-frequency sessions (two to three times per week) over once-weekly visits, especially for motor-based disorders like apraxia and articulation issues.2 As a future SLP, understanding dosage principles will be central to building effective SLP treatment plan strategies.
Third, severity and etiology set the ceiling. A child with a mild phonological delay has a fundamentally different trajectory than an adult recovering from a severe left-hemisphere stroke. Clinicians learn to set realistic, individualized goals rather than promising universal benchmarks.
Understanding Therapy Costs
Cost is a practical concern for clients, and SLPs frequently help families navigate it. Here are current benchmarks:1
Cost per session: Typically ranges from $100 to $250, depending on geographic location, clinical setting, and provider credentials.
Session length: Most sessions last 30 to 60 minutes.
Total course of treatment: For a disorder like an articulation delay requiring roughly 15 to 20 sessions at three times per week, total out-of-pocket costs could range from $1,500 to $5,000 before insurance. Apraxia, requiring 20 to 40 sessions, may run higher.
Insurance coverage: Most private insurance plans and Medicaid cover speech therapy when deemed medically necessary, though session limits and copays vary. School-based services for children are typically provided at no cost under IDEA.
For SLP students, understanding the financial landscape is not just academic. It directly affects treatment planning, client retention, and your ability to advocate for the therapy frequency that research supports. Exploring how different work settings, from hospitals to SLP private practice, influence both your caseload and reimbursement structures will prepare you for the daily realities of clinical work.
The speech-language pathology field has undergone a rapid digital transformation since 2020. From near-universal teletherapy adoption to AI-driven tools and virtual reality rehab platforms, these advances are expanding how SLPs deliver care and creating new specializations for future clinicians to explore.
Frequently Asked Questions About Speech-Language Disorders
Whether you are a prospective speech-language pathology student or simply exploring the field, the questions below address some of the most common inquiries about speech and language disorders, their prevalence, and what treatment looks like in practice. Where specific data is available we have included it, but some prevalence figures are still being refined by ongoing research.
What are the five most common speech disorders?
The five speech disorders clinicians encounter most often are articulation disorders, fluency disorders (such as stuttering), voice disorders, apraxia of speech, and dysarthria. Each affects a different aspect of speech production, from the coordination of oral muscles to the rhythm and quality of the voice. Speech-language pathologists are trained to assess and treat all five, tailoring therapy to the individual's age, severity, and underlying cause.
What famous person has apraxia of speech?
Several public figures have been associated with apraxia of speech. British sports commentator Chris Kamara was diagnosed with apraxia around 2020 and shared his experience in the 2022 documentary Lost For Words. MMA champion Ronda Rousey has spoken about childhood apraxia and credited speech pathologists with helping her overcome it. Comedian Drew Lynch developed apraxia after a sports injury and went on to reach the finals of America's Got Talent Season 10.
What is the 3-1 rule in speech therapy?
The 3-1 rule is a general clinical guideline suggesting that by age three a child's speech should be roughly 75 percent intelligible to unfamiliar listeners. In broader terms, a child's age in years can be multiplied by 25 to estimate the expected intelligibility percentage (for example, 50 percent at age two, 75 percent at age three). When a child falls significantly below these benchmarks, it is typically a signal to seek an evaluation from a speech-language pathologist.
Can mixed receptive-expressive language disorder be cured?
Mixed receptive-expressive language disorder is generally considered a condition that can be significantly improved with targeted therapy rather than fully "cured" in every case. Early, intensive intervention from a speech-language pathologist can help children build comprehension and expressive skills, and many individuals make substantial progress. Outcomes depend on factors like severity, age at the start of therapy, consistency of treatment, and whether the disorder co-occurs with other developmental conditions.
What are the differences in speech disorder prevalence between adults and children?
Speech and language disorders affect both populations but present differently. In children, developmental disorders such as articulation problems, childhood apraxia, and language delays are most common, with estimates suggesting roughly 5 to 10 percent of preschool-age children experience some form of speech or language difficulty. In adults, acquired conditions like aphasia, dysarthria, and voice disorders predominate, often following stroke, brain injury, or neurological disease. Exact prevalence comparisons remain an active area of research.
What are the Big 9 areas of speech-language pathology?
The Big 9, as commonly referenced in SLP education and practice, represent the core areas of clinical focus: articulation, fluency, voice and resonance, receptive language, expressive language, hearing, swallowing (dysphagia), cognitive aspects of communication, and social aspects of communication. These categories help organize the broad scope of practice for speech-language pathologists and are reflected in graduate training, clinical fellowships, and certification requirements.
How long does speech therapy take to show results?
Timelines vary widely depending on the disorder, its severity, and the client's age. Some children with mild articulation errors may show improvement within a few weeks of consistent therapy, while individuals recovering from stroke-related aphasia or managing progressive neurological conditions may require months or even years of ongoing support. Research generally supports that frequency and consistency of practice, both in sessions and at home, are among the strongest predictors of positive outcomes.