E-Stim for Dysphagia: How Electrical Stimulation Works in Speech Therapy
Evidence-based protocols, SLP certification requirements, cost considerations, and when to combine e-stim with traditional swallowing therapy.
By Benjamin Thompson, M.S., CCC‑SLPReviewed by SLP Editoral TeamUpdated August 4, 202625+ min read
Points of interest…
Percutaneous e-stim uses needle electrodes for deeper muscle activation, while transcutaneous devices like VitalStim use surface pads.
Research shows the best dysphagia outcomes when clinicians combine electrical stimulation with traditional swallowing exercises, not as a standalone treatment.
VitalStim certification is a manufacturer training from DJO Global, not an ASHA credential, and is required before administering the device.
E-stim therapy sessions typically bill under specific CPT codes, but coverage varies widely by payer and requires careful documentation.
Electrical stimulation in speech therapy refers to the clinical use of low-level electrical currents to activate or facilitate the muscles involved in swallowing. Unlike e-stim applications in physical therapy or pain management, SLP-directed e-stim targets the suprahyoid and infrahyoid muscle groups central to dysphagia rehabilitation. Three modalities dominate current practice: neuromuscular electrical stimulation (NMES), transcutaneous electrical nerve stimulation (TENS), and percutaneous electrical nerve stimulation (PENS), each differing in electrode placement, depth of stimulation, and intended physiological effect.
The practical challenge for clinicians is straightforward: e-stim devices require manufacturer-specific training that is separate from ASHA certification, reimbursement rules vary by payer and setting, and the evidence base, while growing, still favors e-stim as an adjunct rather than a standalone intervention. For SLP students and early-career professionals exploring speech pathology careers, understanding these constraints is as important as understanding the neuroscience behind the technique.
How Does E-Stim Work for Swallowing and Dysphagia?
Understanding how electrical stimulation supports swallowing rehabilitation starts with a simple chain of events. A clinician places electrodes on the skin of the neck (transcutaneous approach) or inserts thin needle electrodes near the target muscles (percutaneous approach). A controlled electrical current then travels to the motor nerves that supply muscles involved in swallowing. When the current reaches a sufficient intensity, it causes these nerves to depolarize, triggering a muscle contraction. In the context of dysphagia treatment, these contractions target the suprahyoid and infrahyoid muscle groups, the pharyngeal constrictors, and other structures critical to safe, efficient swallowing.
The goal is straightforward: use externally driven contractions to strengthen muscles that may be weakened or discoordinated following stroke, head and neck cancer treatment, traumatic brain injury, or progressive neurological disease. Dysphagia is one of the most clinically significant speech-language disorders, and e-stim offers a powerful tool for addressing it.
Sensory-Level vs. Motor-Level Stimulation
Not every e-stim session aims for a visible muscle contraction. Clinicians distinguish between two intensity thresholds, and the choice depends on the clinical picture.
Sensory-level stimulation: The current is set below the motor threshold. The patient feels a tingling sensation, but no visible contraction occurs. This approach is used to heighten sensory awareness in the pharynx and larynx, which can improve swallow timing and initiation in patients whose primary deficit is reduced sensation rather than muscle weakness.
Motor-level stimulation: The current intensity is raised until it produces a palpable or visible muscle contraction. This level is appropriate when the treatment goal is muscle strengthening, improved hyolaryngeal excursion, or increased pharyngeal squeeze.
Selecting the right level is a clinical decision informed by instrumental assessment findings such as videofluoroscopic swallow studies or fiberoptic endoscopic evaluation of swallowing.
The Neuroplasticity Connection
Electrical stimulation does more than simply contract muscles. When a patient performs volitional swallow exercises at the same time the current activates the target muscles, the paired activity sends simultaneous signals through both peripheral and central neural pathways. Over repeated sessions, this dual input promotes cortical reorganization, essentially encouraging the brain to recruit new neural circuits to compensate for damaged areas. This neuroplasticity mechanism is a key reason e-stim is considered especially promising for stroke-related dysphagia, where the brain retains some capacity to rewire motor pathways.
An Adjunct, Not a Standalone
It is worth noting early that e-stim is almost always used alongside traditional swallowing exercises rather than as a standalone intervention. Techniques like effortful swallows, the Mendelsohn maneuver, and resistance-based lingual exercises remain central to dysphagia rehabilitation. E-stim adds an additional stimulus that may accelerate gains, but it does not replace the active, volitional effort that drives long-term functional improvement. Most current clinical protocols reflect this philosophy, pairing electrical stimulation with individualized exercise programs tailored to each patient's specific swallowing impairments. SLPs working in acute care or inpatient rehab speech pathology settings are among the most frequent users of these combined protocols.
Percutaneous Vs. Transcutaneous Electrical Stimulation for Dysphagia
When clinicians discuss e-stim for dysphagia, two distinct delivery methods come into play: transcutaneous electrical stimulation (TES), which uses surface electrode pads placed on the skin, and percutaneous electrical stimulation (PES), which involves needle or fine-wire electrodes inserted directly into the target muscle tissue.1 Understanding how these approaches differ is essential for SLPs weighing treatment options and for students learning the clinical reasoning behind each choice.
How Electrode Delivery Differs
Transcutaneous stimulation relies on surface electrode pads, typically ranging from two to five square centimeters, positioned on the skin overlying the muscles of interest.2 The current passes through skin, subcutaneous fat, and connective tissue before reaching the muscle, so its effective depth is relatively superficial. This approach is non-invasive, well tolerated by most patients, and can be administered by a trained SLP or even guided for home-program use in some protocols.
Percutaneous stimulation, by contrast, places hypodermic or fine-wire needle electrodes directly at the motor points of target muscles.3 Because the current is delivered at the muscle itself, depth penetration is high, and the clinician can activate structures that surface pads simply cannot reach effectively. However, this invasiveness raises the risk profile and typically requires physician involvement for electrode placement.
Which Muscles Can Each Method Target?
This distinction in depth is clinically meaningful. Surface e-stim generally targets the suprahyoid group and accessible thyrohyoid or infrahyoid muscles.4 Percutaneous stimulation can reach deeper structures such as the geniohyoid, mylohyoid, digastric, sternohyoid, omohyoid, thyrohyoid, and pharyngeal constrictors.3 For patients whose dysphagia stems from weakness in these deeper muscles, surface stimulation alone may not generate enough neuromuscular recruitment to produce functional change. This is an important consideration within the broader SLP scope of practice, where clinicians must match intervention intensity to each patient's presentation.
Candidacy and Outcome Considerations
Transcutaneous e-stim is generally appropriate for patients with mild to moderate oropharyngeal dysphagia.2 It carries a low risk profile and integrates smoothly into standard outpatient therapy sessions. Percutaneous stimulation tends to be reserved for patients with severe dysphagia who have shown a poor response to surface e-stim.3 Some studies have reported stronger hyolaryngeal excursion gains with percutaneous delivery, likely because the current reaches the precise motor points driving hyoid elevation and laryngeal closure. Guidance from NICE on transcutaneous neuromuscular electrical stimulation for oropharyngeal dysphagia, along with meta-analytic work on optimal electrode placement for dysphagia, helps frame where each modality fits in the evidence hierarchy.
Practical Factors for Clinicians
Setting matters. Transcutaneous e-stim is feasible in outpatient clinics, skilled nursing facilities, and even some home health contexts. Percutaneous procedures typically occur in medical centers or hospital-based outpatient settings where a physician can place electrodes and monitor for complications such as localized bleeding or infection. Patient tolerance is another consideration: some individuals find needle insertion uncomfortable, which can affect adherence over a multi-session treatment course. Session durations for both modalities generally fall within a similar range, though percutaneous sessions may require additional time for electrode placement and post-procedure monitoring.
Surface (transcutaneous): Non-invasive, low risk, administered by the SLP, best suited for mild to moderate dysphagia in outpatient or community settings.2
Needle (percutaneous): Invasive, higher risk, requires physician collaboration, targets deeper musculature, and is typically reserved for severe cases unresponsive to surface stimulation.3
For SLP students and early-career clinicians, understanding these two pathways is not just academic. The choice between transcutaneous and percutaneous delivery shapes treatment planning, interdisciplinary collaboration, required certifications, and the clinical settings where you may practice.
Questions to Ask Yourself
Does the patient have intact peripheral nerve supply to the targeted swallowing muscles?
E-stim relies on nerve pathways to activate muscle contraction. If lower motor neurons are severely damaged or absent, the electrical current cannot produce a meaningful therapeutic response, and alternative approaches may be more appropriate.
Has the patient plateaued with traditional swallowing exercises alone?
E-stim is typically introduced as an adjunct when conventional dysphagia therapy stops producing measurable gains. Documenting a plateau strengthens clinical justification and supports insurance authorization for adding electrical stimulation.
Does the patient have a cardiac pacemaker, implanted defibrillator, carotid stent, or active cancer in the cervical region?
Each of these conditions is a recognized contraindication. Electrical current near a pacemaker can disrupt cardiac rhythm, stimulation over a carotid stent risks vascular complications, and e-stim in a region with active malignancy may promote abnormal tissue growth.
Is the patient cognitively and physically able to participate in active swallowing trials during stimulation?
Research consistently shows better outcomes when e-stim is paired with volitional swallowing practice rather than applied passively. Patients who cannot follow simple commands or tolerate repeated swallow attempts may not benefit from this modality.
Vitalstim, Omnistim FX2, and E-Stim Device Comparison
Choosing the right electrical stimulation device is a clinical decision that hinges on treatment goals, electrode type, facility resources, and the training available to the treating SLP. Three devices dominate the conversation in dysphagia rehabilitation: VitalStim, Omnistim FX2, and Ampcare ESP. Each occupies a slightly different niche, and understanding their differences will help you make informed choices as you move into clinical practice.
VitalStim: The Industry Standard
VitalStim is the most widely recognized neuromuscular electrical stimulation (NMES) device in speech-language pathology. It is FDA-cleared specifically for the treatment of dysphagia and uses a dual-channel, surface electrode system that delivers low-level electrical current through pads placed on the anterior neck. Clinicians pair the stimulation with traditional swallowing exercises to promote muscle re-education.
What sets VitalStim apart from competitors is not just its regulatory clearance but its branded SLP certification pathway. Clinicians must complete a dedicated training course before using the device, and this structured credentialing process has driven widespread adoption across hospitals, skilled nursing facilities, and outpatient clinics. Because the certification is well established, many employers specifically look for SLPs who hold VitalStim credentials, which in turn reinforces the device's market dominance. For a broader look at how specialty credentials shape your career, see our guide to SLP additional certifications.
Omnistim FX2: Percutaneous Capability
The Omnistim FX2 offers a broader range of stimulation parameters and, critically, supports percutaneous electrode delivery in addition to surface stimulation. Percutaneous electrodes are fine-wire needles inserted into or near target muscles, allowing the current to reach deeper pharyngeal and laryngeal structures that surface pads cannot easily access. This makes the Omnistim FX2 a compelling option in research settings and specialized dysphagia clinics where percutaneous protocols are part of the treatment plan. Its versatility appeals to clinicians who want a single device capable of both transcutaneous and percutaneous approaches, though the percutaneous component requires additional training and is not as commonly used in everyday clinical settings.
Ampcare ESP: Submental Focus
Ampcare ESP takes a more targeted approach by concentrating stimulation on the submental muscle group, the muscles beneath the chin that play a central role in hyolaryngeal elevation during swallowing. The device pairs its electrical stimulation with a guided exercise protocol designed to strengthen these specific muscles. For patients whose primary deficit involves reduced hyoid excursion or impaired laryngeal elevation, Ampcare ESP offers a focused treatment option. Its narrower scope can be an advantage when the clinical picture clearly points to submental weakness, but it may be less versatile for patients who need broader pharyngeal stimulation.
How to Decide Between Devices
Device selection depends on several interrelated factors:
Treatment goals: If the aim is general pharyngeal muscle re-education with surface electrodes, VitalStim is the most straightforward choice. For targeted submental strengthening, Ampcare ESP is purpose-built. For deeper muscle access via percutaneous electrodes, the Omnistim FX2 is the primary option.
Electrode type: Surface electrodes are noninvasive and easier to administer, making them practical in most clinical environments. Percutaneous electrodes require specialized training and sterile technique, limiting their use to facilities equipped for that level of intervention.
Certification and training access: VitalStim's established certification pathway makes it the easiest device to get trained on and the most likely to be recognized by employers. Training pathways for the Omnistim FX2 and Ampcare ESP exist but are less standardized across the profession.
Facility resources: Budget, available training time, and patient population all influence which device a clinic adopts. A skilled nursing facility treating primarily stroke patients may default to VitalStim, while a university medical center conducting dysphagia research might invest in the Omnistim FX2.
As you pursue your SLP education and begin speech pathology internship placements, you will likely encounter VitalStim first. Gaining familiarity with all three devices, even at a conceptual level, positions you to advocate for the best tool for each patient rather than defaulting to whatever happens to be on the shelf.
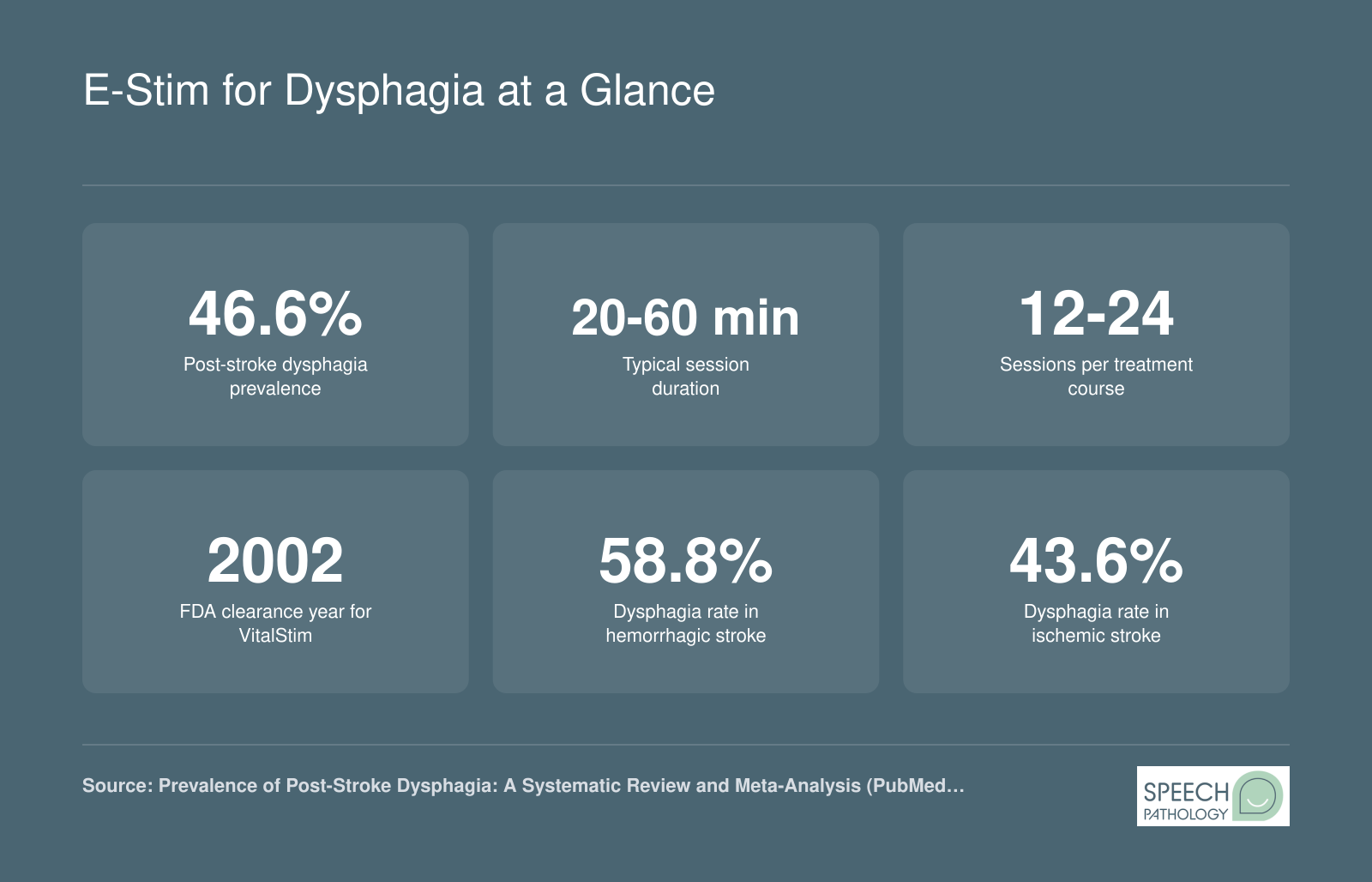
E-Stim for Dysphagia at a Glance
Electrical stimulation therapy for dysphagia involves a structured treatment course supported by growing clinical evidence. Here are the key numbers every SLP student and clinician should know.
Evidence Base: Research Outcomes and Success Rates (2024-2026 Update)
The evidence supporting neuromuscular electrical stimulation (NMES) for dysphagia has matured significantly over the past several years. If you are planning a career in speech-language pathology, understanding the current research landscape will help you make informed clinical decisions and counsel patients with realistic expectations.
Post-Stroke Dysphagia: The Strongest Evidence
Stroke-related dysphagia remains the population where NMES shows the most compelling results. A 2025 network meta-analysis published in *Frontiers in Neurology* reported a Cohen's d effect size of 0.88 for NMES in post-stroke dysphagia, which is considered a large clinical effect.1 Patients demonstrated approximately 15% improvement in upper esophageal sphincter opening, along with measurable gains in laryngeal elevation, thyrohyoid muscle strength, and overall dietary intake.2 Functional brain imaging (fMRI) studies have also confirmed that NMES can enhance cortical activation patterns, supporting the theory that the treatment works through neuromuscular re-education rather than simple muscle strengthening alone.1 Quality-of-life measures improved as well, reinforcing that the functional gains carry over into daily eating and drinking.
A separate meta-analysis of six randomized controlled trials examining transcranial electrical stimulation (a related modality sometimes used alongside peripheral NMES) found a statistically significant overall effect size of 0.43, with low-intensity protocols (effect size 0.46) slightly outperforming high-intensity ones (0.37).3 This suggests that more stimulation is not always better, an important nuance for clinicians selecting treatment parameters.
Head and Neck Cancer and Neurodegenerative Conditions: Mixed Results
The picture is less clear for other etiologies. For patients with dysphagia secondary to head and neck cancer, the 2025 evidence rates NMES efficacy as limited.1 Radiation-induced fibrosis and tissue changes may reduce the responsiveness of muscles to electrical stimulation, making traditional swallowing exercises and compensatory strategies more central for this population.
Similarly, individuals with neurodegenerative conditions such as Parkinson's disease, ALS, or multiple sclerosis have limited evidence supporting NMES.2 The progressive nature of these diseases means that gains, when they occur, may be temporary. However, some clinicians report that NMES can slow functional decline or maintain swallowing safety for longer periods when combined with active exercise programs. Larger, well-designed trials are needed before firm clinical recommendations can be made for these groups.
Pediatric Populations: Promising Early Data
One encouraging development is the emerging research in pediatric dysphagia. Studies from 2025 report that NMES improved suprahyoid muscle activation and overall swallowing efficiency in children.1 Perhaps the most striking finding is a reduction in tube-feeding dependency ranging from 70% to 100% in certain pediatric cohorts. While these results are preliminary and drawn from small samples, they suggest a population that may benefit substantially from further investigation.
Addressing Earlier Criticisms and Study Limitations
Older Cochrane-era reviews frequently noted that the evidence for NMES in dysphagia was inconclusive. These criticisms were valid at the time: many early studies used small sample sizes, lacked assessor blinding, and varied widely in stimulation protocols, electrode placement, and outcome measures. The newer generation of research has improved on these fronts, with more randomized controlled trials, standardized outcome tools (such as the Swallowing Status Assessment, which showed a mean difference of negative 6.43 points favoring NMES in mixed dysphagia populations), and better-defined treatment parameters.1
That said, significant limitations persist.4 Sample sizes in many studies remain small, protocol heterogeneity across research centers makes direct comparisons difficult, and assessor blinding is still lacking in a number of trials. The safety profile of NMES is reassuring, with only minor adverse effects reported, but the field has not yet reached the level of evidence that would support NMES as a standalone treatment.5
Long-Term Maintenance of Gains
One of the most important clinical questions is whether treatment gains persist after NMES sessions end. Unfortunately, long-term maintenance data remains a critical gap in the literature.4 While some stroke studies have tracked patients for several weeks post-treatment and found sustained improvement, robust data at three to six months is sparse. Clinicians should set patient expectations accordingly and plan for ongoing monitoring and, when needed, booster sessions or continued traditional swallowing exercises.
For students and early-career SLPs, the takeaway is straightforward: NMES for dysphagia is supported by growing and increasingly rigorous evidence, particularly for post-stroke patients. It is appropriately classified as an adjunctive therapy, meaning it works best when layered on top of, not in place of, traditional swallowing rehabilitation. Grounding your practice in evidence-based practice in speech-language pathology and staying current through resources like the ASHA Evidence Map for NMES and dysphagia and peer-reviewed journals will serve you well as this field continues to evolve.
Patient Candidacy, Contraindications, and Safety Protocols
Electrical stimulation for dysphagia can be a valuable clinical tool, but it is not appropriate for every patient. Careful screening for candidacy, awareness of contraindications, and adherence to established safety protocols are essential before initiating treatment. The following guidelines draw from device manufacturer recommendations and clinical practice standards.1
Who Is a Good Candidate?
Not every patient with dysphagia will benefit from e-stim. Strong candidates generally meet several criteria:
Intact lower motor neuron supply: The targeted muscles must have a functioning nerve supply so they can respond to electrical current. Muscles that are fully denervated will not contract meaningfully with surface or percutaneous stimulation.
Identifiable muscle targets: The clinician should be able to locate and access the specific muscles contributing to the swallowing deficit. This typically requires a thorough instrumental assessment, such as a videofluoroscopic swallow study or fiberoptic endoscopic evaluation, before treatment begins.
Active patient participation: E-stim works best when paired with volitional swallowing exercises. Patients who are motivated, alert, and able to follow directions during sessions tend to achieve better outcomes.
Documented oropharyngeal dysphagia: VitalStim received FDA clearance in 2001 specifically for oropharyngeal dysphagia, so the diagnosis should be confirmed through objective evaluation rather than clinical screening alone.2
Absolute Contraindications
Certain conditions make electrical stimulation unsafe. Clinicians should never apply e-stim in the presence of:
A demand-type cardiac pacemaker or implanted cardiac defibrillator, because the external current may interfere with device function.1
A carotid sinus stimulator or any implanted neurostimulation device in the cervical region.
Electrode placement directly over the carotid artery, which risks triggering a vasovagal response or dangerous changes in heart rate and blood pressure.
An active neoplasm or infection at the intended stimulation site, as stimulation could worsen the underlying condition or spread the disease process.1
Relative Contraindications and Precautions
Some conditions do not automatically rule out e-stim but require additional clinical judgment and potentially physician clearance:
Seizure history: Cervical stimulation in patients with a seizure disorder warrants careful risk-benefit analysis and medical team coordination.
Pregnancy: The effects of cervical electrical stimulation on a developing fetus have not been adequately studied, so most protocols advise against treatment.
Active malignancy in the cervical area: Even when the tumor is not directly at the electrode site, nearby malignancy raises concerns about promoting cell growth or spreading disease.
Metal implants near electrode sites: Hardware such as cervical spine fixation plates can alter current pathways in unpredictable ways, increasing the risk of burns or ineffective stimulation.
Regardless of the clinical scenario, the clinician must discontinue treatment immediately if there is any sign of device interference, unexpected pain, or skin irritation at the electrode site.1
Pediatric Considerations
The evidence base for e-stim in pediatric dysphagia remains limited.3 There is no established minimum age threshold, but several factors complicate its use with younger patients:4
Smaller cervical anatomy demands modified electrode placement. Standard adult configurations simply do not translate to a child's neck.
Stimulation amplitude is typically reduced by 50 to 70 percent compared with adult settings, and session duration is generally shortened to 20 to 30 minutes.4
Parental consent, cooperation, and the child's ability to tolerate the sensation of stimulation all influence whether treatment is feasible.
Randomized controlled trials in pediatric populations are scarce, so clinicians should rely on careful clinical reasoning, close monitoring, and transparent discussions with families about the current evidence gaps.3
If you are considering a career path focused on younger populations, learning about how to become a pediatric speech pathologist can help you understand the specialized training these cases require.
Before initiating e-stim with any patient, whether adult or pediatric, a thorough review of medical history and direct communication with the referring physician can help ensure safe, appropriate treatment. Completing a comprehensive SLP evaluation and treatment planning process, and documenting the screening rationale for candidacy decisions, is equally important for protecting the patient and the clinician.
Did You Know?
Current evidence and clinical guidelines consistently position electrical stimulation as a complement to traditional swallowing therapy exercises, including the effortful swallow, Mendelsohn maneuver, and Shaker exercises, rather than a standalone intervention. Research shows that the best patient outcomes occur when clinicians use combined protocols that pair e-stim with active exercise programs tailored to each individual's swallowing deficit.
SLP Certification and Training Requirements for E-Stim
One of the most common misconceptions among student clinicians and early-career SLPs is that VitalStim certification is an ASHA credential. It is not. VitalStim certification is a manufacturer-provided training program administered by DJO Global (the company that produces VitalStim devices). ASHA does not grant, endorse, or regulate any specific e-stim certification. Understanding this distinction matters because it shapes how you present the credential on a resume and how employers evaluate your qualifications.
What ASHA's Scope of Practice Actually Says
ASHA recognizes that the use of electrical stimulation for dysphagia falls within the scope of practice for speech-language pathologists. This means that a fully licensed SLP is permitted to integrate e-stim into swallowing treatment plans, provided they have the requisite knowledge and competency. However, ASHA leaves the specifics of training and credentialing to individual practitioners, employers, and state licensure boards. Some state boards impose additional requirements, such as documented supervised clinical hours with e-stim devices or completion of a board-approved training course, before an SLP may bill for or administer electrical stimulation therapy. Always check your state's licensure board website for the most current rules.
The Typical Certification Pathway
Most SLPs pursue VitalStim certification because it is widely recognized by employers and insurance carriers. The pathway generally includes the following steps:
Online didactic coursework: Covers anatomy of the swallowing mechanism, electrode placement protocols, contraindications, and device operation. This portion can usually be completed at your own pace.
Hands-on clinical training: A live or in-person practicum component where you practice electrode placement, parameter settings, and patient assessment under instructor supervision. This typically takes one to two days.
Competency examination: A written or practical exam verifying your ability to safely and effectively administer treatment.
Continuing education credits: Completion of VitalStim training typically awards ASHA-approved CEU credits, which count toward your ongoing professional development requirements.
Cost and Time Commitment
Expect to invest roughly $500 to $1,000 for the full VitalStim certification program, depending on the training provider and whether in-person workshops are included. The total time commitment is usually one to two days for the hands-on portion, plus several hours of independent online study. Some employers cover part or all of the cost, so it is worth asking during the hiring process or requesting professional development funding from your facility.
Practical Advice for Students
If you are still in graduate school, you likely will not pursue e-stim certification until after you have earned your CCC-SLP certification. Most certification programs require participants to hold a current SLP license. That said, familiarizing yourself with the evidence base and observing e-stim sessions during clinical placements will put you in a stronger position to pursue certification early in your career. Employers in medical settings, particularly acute care hospitals and skilled nursing facilities, often view VitalStim certification as a desirable medical SLP certification that can set you apart from other candidates.
For more guidance on building clinical specializations and navigating post-graduate training, explore resources that map out career pathways in how to become a speech-language pathologist.
Cost, Insurance, CPT Codes, and Reimbursement for E-Stim Therapy
Understanding the financial side of electrical stimulation therapy is essential whether you are a student preparing for clinical practice or a working SLP navigating reimbursement for the first time. Billing for e-stim in dysphagia treatment involves specific procedure codes, payer-specific rules, and careful documentation. Below is a practical breakdown of what you need to know.
Key CPT Codes for E-Stim Billing
Two Current Procedural Terminology (CPT) codes come up most often when billing for e-stim dysphagia sessions:
CPT 97032 (Electrical Stimulation, Attended): This code covers the application of electrical stimulation that requires direct, one-on-one contact with the clinician. It is time-based and billed in 15-minute units. SLPs use this code when the primary service rendered during that portion of the session is the electrical stimulation itself.
CPT 92526 (Treatment of Swallowing Dysfunction): This code covers therapeutic intervention for swallowing disorders and is not time-based; it is billed per session. When an SLP combines traditional swallowing exercises with e-stim in the same visit, both codes may be reported.
A critical point for Medicare billing: the Centers for Medicare and Medicaid Services (CMS) may bundle these codes under certain circumstances. If both are billed on the same date of service, documentation must clearly distinguish the time and therapeutic purpose of each intervention. Without that separation, the claim risks denial or downcoding. Always check the latest National Correct Coding Initiative (NCCI) edits to confirm whether a modifier (such as Modifier 59 for distinct procedural services) is appropriate.
Typical Cost Per Session and Full Treatment Course
Out-of-pocket costs for a single e-stim session generally range from $75 to $250, depending on the clinical setting, geographic region, and payer. Hospital outpatient departments tend to charge at the higher end, while SLP private practice settings and skilled nursing facilities may fall toward the middle or lower range.
A full treatment course typically spans 12 to 24 sessions, sometimes more depending on severity and patient response. That puts the total cost of a complete e-stim treatment plan in the range of $900 to $6,000. For patients without insurance coverage, this can represent a significant financial commitment, so discussing costs early in the plan of care helps set realistic expectations.
Medicare Coverage and Documentation Requirements
CMS does cover neuromuscular electrical stimulation (NMES) for dysphagia when the service is deemed medically necessary. However, denials are common, and they almost always trace back to insufficient documentation. Medicare requires clear evidence that the patient has a diagnosed swallowing disorder, that the treatment plan is individualized, and that the intervention is expected to produce meaningful functional improvement within a reasonable timeframe.
To strengthen a Medicare claim, your documentation should include:
Objective findings from a Fiberoptic Endoscopic Evaluation of Swallowing (FEES) or a Modified Barium Swallow Study (MBSS)
Specific functional goals tied to swallowing safety or diet advancement
A physician order or referral supporting the medical necessity of e-stim
Vague language such as "patient tolerated treatment well" is not enough. Payers want to see quantifiable outcomes, such as changes in penetration-aspiration scale scores, improvements in hyolaryngeal excursion, or documented diet upgrades.
Tips for Private Insurance and Handling Denials
Private insurers vary widely in their coverage policies for e-stim in dysphagia. Some cover it readily under speech therapy benefits; others classify it as experimental or investigational, particularly for certain diagnoses. A few practical steps can improve your chances of approval:
Obtain pre-authorization: Before initiating treatment, contact the insurer to verify coverage and request pre-authorization if required. This single step prevents many downstream denials.
Submit a letter of medical necessity: Reference instrumental assessment findings from FEES or MBSS, describe the patient's functional limitations, and explain why traditional therapy alone is insufficient.
Appeal initial denials: First-round denials are not uncommon, but they are often overturned on appeal. Include peer-reviewed literature supporting e-stim efficacy for the patient's specific condition and attach updated clinical documentation.
For students and early-career SLPs working toward their CCC-SLP certification, gaining familiarity with the reimbursement landscape now will serve you well. Effective clinical documentation is not just a billing skill; it is how you advocate for your patients' access to the treatments they need.
Frequently Asked Questions About E-Stim in Speech Therapy
Electrical stimulation for dysphagia is a rapidly evolving area of speech-language pathology practice. Below, we answer the most common questions students and early-career SLPs have about how e-stim works, certification requirements, costs, and clinical evidence.
How does electrical stimulation help with swallowing disorders?
Electrical stimulation delivers small, controlled currents to the muscles involved in swallowing. This stimulation can strengthen weakened pharyngeal and laryngeal muscles, improve hyolaryngeal elevation, and promote cortical reorganization (neuroplasticity). When combined with active swallowing exercises, the added sensory and motor input helps patients retrain coordinated swallow patterns more effectively than exercise alone in many cases.
What is the difference between percutaneous and transcutaneous electrical stimulation?
Transcutaneous electrical stimulation (such as VitalStim) delivers current through surface electrodes placed on the skin. Percutaneous electrical stimulation uses thin, needle-like electrodes inserted through the skin directly into or near the target muscles. Percutaneous approaches allow more precise muscle targeting and potentially stronger contractions, but they are more invasive and typically require additional clinical training and medical oversight compared to surface electrode methods.
Do SLPs need special certification to use VitalStim?
Yes. SLPs must complete a manufacturer-approved VitalStim certification course before administering VitalStim therapy. This training covers electrode placement protocols, patient selection, contraindications, and device operation. The certification program typically involves an online or in-person course followed by a competency assessment. Many employers and insurance payers require proof of current VitalStim certification before an SLP can bill for this service.
What CPT code is used for electrical stimulation in speech therapy?
The most commonly used CPT code for neuromuscular electrical stimulation in dysphagia therapy is 97014 (unattended electrical stimulation) or 97032 (attended electrical stimulation). Some clinicians also bill 92526 for the swallowing therapy component performed alongside the stimulation. Exact coding depends on payer guidelines, whether the SLP is present throughout, and the clinical setting. Always verify current requirements with each insurance carrier.
Is electrical stimulation effective for dysphagia caused by stroke?
Research shows promising results for stroke-related dysphagia, particularly when e-stim is used as an adjunct to traditional swallowing exercises during the subacute recovery phase. Several studies report improved Penetration-Aspiration Scale scores and increased hyoid bone movement. However, outcomes vary depending on stroke severity, time since onset, and patient compliance. E-stim appears most effective when integrated into a comprehensive, individualized treatment plan rather than used in isolation.
How much does e-stim therapy cost per session?
E-stim therapy sessions for dysphagia generally range from $100 to $350 per session, depending on the clinical setting, geographic location, and whether the treatment is provided in an outpatient clinic or hospital. Insurance coverage varies widely by payer and plan. Medicare and many private insurers may cover e-stim under specific conditions when medical necessity is documented, though prior authorization is often required.
How many e-stim sessions are typically needed for dysphagia treatment?
Most treatment protocols involve 12 to 24 sessions, often scheduled three to five times per week over several weeks. The exact number depends on the severity and etiology of the dysphagia, how the patient responds to initial sessions, and the treatment goals established during the evaluation. Clinicians reassess progress using instrumental swallowing studies (such as FEES or modified barium swallow) to determine when therapy goals have been met or when the plan needs adjustment.