How OAE Screening Works: Equipment, Procedure, and Pass/refer Criteria
Understanding the mechanics of an otoacoustic emissions screening helps speech-language pathologists feel confident when administering the test, explaining results to caregivers, and determining next steps. The process is quick, noninvasive, and does not require the individual being screened to respond behaviorally, which is one reason it is so widely used with newborns and young children.
Step-by-Step Screening Procedure
A typical OAE screening follows a straightforward sequence that takes roughly one to three minutes per ear:
- Select an ear tip: Choose the appropriately sized disposable ear tip or probe tip. A snug, sealed fit in the ear canal is essential for accurate results; an improper seal is one of the most common causes of a false refer.
- Insert the probe: Gently place the probe into the ear canal. The probe houses both a miniature speaker (to deliver the sound stimulus) and a sensitive microphone (to pick up the emissions returning from the cochlea).
- Deliver the stimulus: The device sends a controlled acoustic stimulus into the ear canal. The outer hair cells of a healthy cochlea respond by producing their own faint sounds, which travel back through the middle ear and into the ear canal.
- Record and analyze emissions: The probe microphone captures the returning emissions, and the screening device analyzes them automatically against built-in criteria.
The person being screened does not need to raise a hand or press a button. This makes OAE screening especially practical for infants, toddlers, and individuals who may have difficulty participating in behavioral hearing tests.
Two Main Stimulus Types: TEOAEs and DPOAEs
Screening devices use one of two stimulus approaches, and each has distinct strengths.
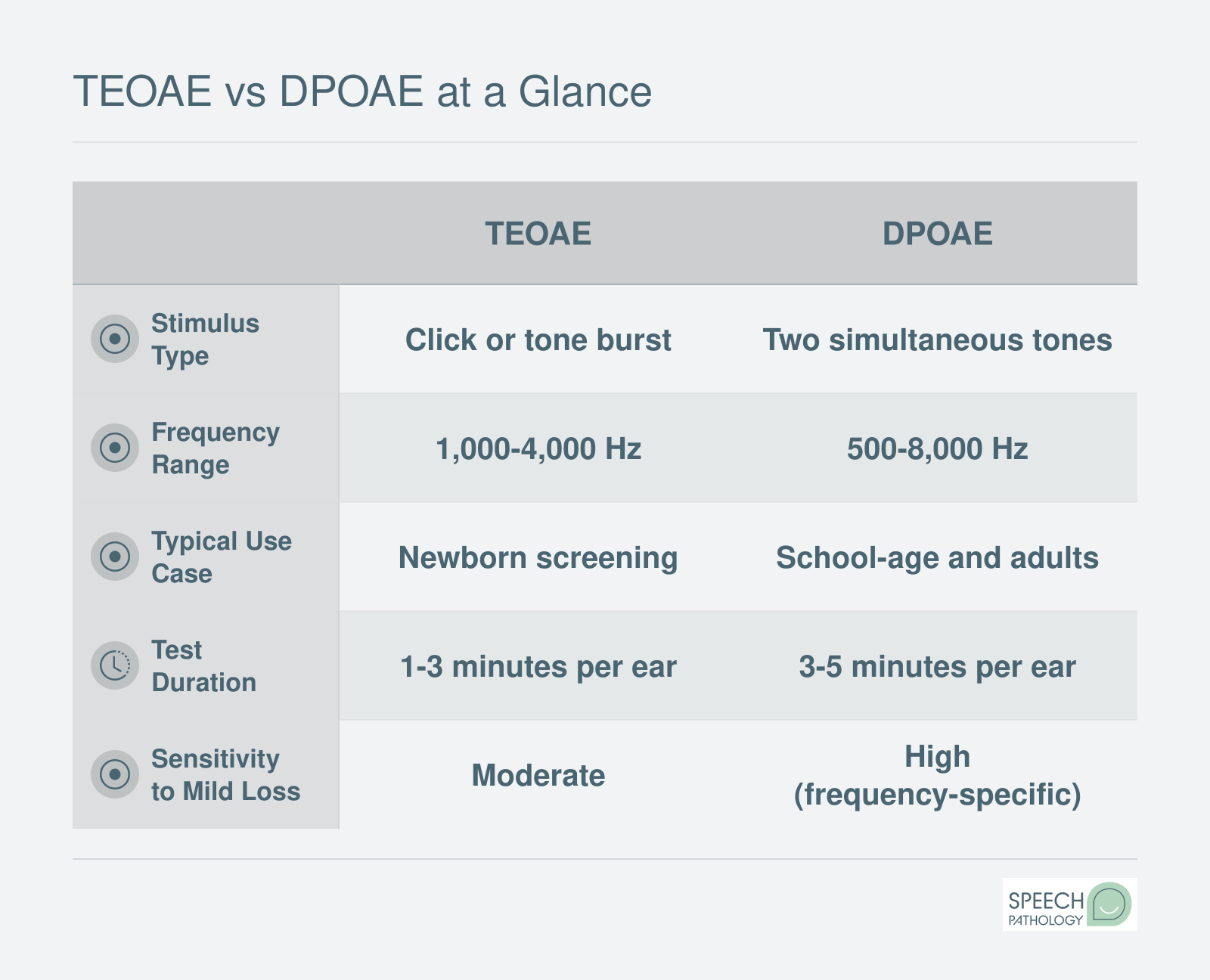
Transient evoked otoacoustic emissions (TEOAEs) use a broadband click stimulus. The cochlea responds across a range of frequencies, typically covering roughly 1,000 to 4,000 Hz. TEOAEs are widely used in newborn hearing screening programs because they provide a fast, global snapshot of outer hair cell function across the speech-frequency range.
Distortion product otoacoustic emissions (DPOAEs) use two simultaneous pure tones presented at slightly different frequencies. The cochlea produces a measurable distortion product at a mathematically predictable frequency. DPOAEs allow frequency-specific testing across a broader range, typically from about 1,000 to 8,000 Hz. This makes DPOAEs particularly useful when a clinician wants to evaluate cochlear function at specific frequencies, such as the higher frequencies that are often affected early in noise-induced or ototoxic hearing loss.
Some screening programs and clinics prefer one type over the other based on the population served and the clinical question at hand.
Pass/Refer Criteria
OAE screening devices are designed to produce a clear outcome: pass or refer. The device determines this by evaluating the signal-to-noise ratio (SNR) at each tested frequency band. A pass generally requires an SNR of at least 6 dB across specified frequency bands, indicating that the cochlear emissions are clearly distinguishable from background noise.
A refer result means that emissions were absent, too weak, or could not be detected above the noise floor at one or more frequencies. A refer does not automatically confirm hearing loss. It signals that further evaluation is needed, often through a diagnostic audiological assessment.
Understanding the Normal Range
In a research or diagnostic context, OAE amplitudes typically fall somewhere between negative 10 and positive 20 dB SPL, depending on the frequency tested, the individual's age, and the device used. However, SLPs conducting screenings should understand that most screening-level OAE devices do not display raw amplitude data. Instead, they simplify the output to a pass or refer designation.
This distinction matters. SLPs new to OAE screening sometimes expect to see a number they can compare to a threshold, similar to a pure-tone audiogram. OAE screeners work differently. The internal algorithm handles the comparison, so the clinician's job is to ensure proper probe placement, a quiet testing environment, and an accurate recording of the result. If a screening device does display amplitude or SNR data, the SLP should use it to confirm the pass/refer outcome rather than to diagnose the type or degree of hearing loss, which falls within the audiologist's scope of practice.
OAE screening results often feed into broader SLP evaluation and treatment planning workflows, especially when hearing status may be influencing speech or language development. By understanding how the equipment works and what the results mean, SLPs can play a valuable role in identifying individuals who need audiological follow-up, all while staying within their professional boundaries.